Ocular siderosis (Ocular Siderosis / Siderosis bulbi) is a disease that occurs when an intraocular foreign body (IOFB) containing iron or iron alloy remains inside the eye. The retained iron dissolves into the eye tissues, and iron ions damage the cornea, iris, lens, retina, trabecular meshwork, and other ocular tissues. The concept of this disease was first described by Bunge in 1860. It is a rare disease with a prevalence of about 0.002% among patients with eye injuries. 1)
Ocular chalcosis (Ocular Chalcosis) is a disease caused by a retained copper-containing IOFB. Copper ions deposit in various eye tissues and cause characteristic tissue damage. If pure copper (more than 90% copper) remains, it presents as an acute form with a severe endophthalmitis-like reaction. Low-copper alloys such as brass take a chronic, slowly progressive course.
IOFB can remain in the eye without symptoms at first and gradually cause progressive tissue damage, so delayed diagnosis markedly worsens the visual prognosis. Magnetic materials (iron and steel) account for 30–40% of all intraocular foreign bodies, and copper-alloy foreign bodies are relatively rare.
QCan metals other than iron also cause problems inside the eye?
A
With copper-containing intraocular foreign bodies, severe ocular chalcosis occurs, just like siderosis. Pure copper causes an acute endophthalmitis-like reaction, while brass causes a chronic deposition disorder. Aluminum and glass cause only mild tissue reactions and are distinguished from siderosis and chalcosis.
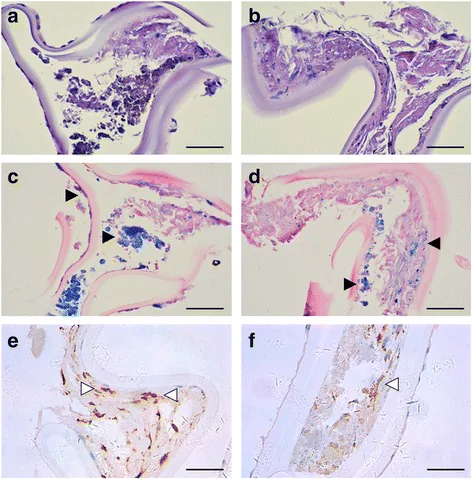
Zhang KK, He WW, Lu Y, et al. Siderotic cataract with no signs of intraocular foreign body. BMC Ophthalmol. 2017;17(1):26. Figure 5. PMID: 28288588; PMCID: PMC5348785; DOI: 10.1186/s12886-017-0424-4. License: CC BY.
Histopathological findings of the anterior lens capsule in ocular siderosis. HE staining (a, b) shows hemosiderin deposition, Prussian blue staining (c, d) shows accumulation of iron pigment, and infiltration of CD18-positive macrophages (e, f) is seen in the anterior capsule. This corresponds to the siderotic cataract discussed in the section ‘Main symptoms and clinical findings’.
Symptoms of siderosis are divided into those that appear immediately after the injury and those that gradually progress after the foreign body remains.
Decreased vision: the most common symptom, seen in about 63.79% of patients.1)
Asymptomatic: In the early stage, symptoms are minimal, and about 27.58% of patients are found without any symptoms.1)
Night blindness and visual field narrowing: These appear as selective damage to rod cells progresses.
Eye pain and redness: Seen in the acute phase of IOFB injury or when inflammation is present.
Corneal iron deposition: Iron deposits in the epithelium or stroma. Seen in about 46.55% of patients.1)
Siderotic mydriasis (mydriasis siderostica): A characteristic dilated pupil caused by iron damage to the iris sphincter muscle.3)
Siderotic cataract: A characteristic brown clouding beneath the anterior lens capsule. Seen in about 37.93% of patients.1)
Retinal pigment epithelium (RPE) degeneration: The most common finding, seen in about 72.41% of patients.1)
Eye findings in chalcosis
Kayser-Fleischer ring-like change: A yellow-green ring-like change caused by copper deposition at the corneal limbus (Descemet’s membrane). Characteristic of the chronic type.
Emerald ring: A green ring-like clouding beneath the anterior lens capsule. A characteristic pathological finding of chalcosis.
Acute findings (pure copper): severe endophthalmitis-like inflammation, hypopyon, and vitreous opacification.
Siderotic glaucoma is an important complication. Iron deposition in the trabecular meshwork can cause secondary open-angle glaucoma4).
QWhat is affected first in siderosis?
A
ERG findings show that rods are selectively affected early. Reduced b-wave amplitude appears first, followed by reduced a-wave amplitude and eventually a flat electroretinogram. See the pathophysiology section for details.4)
The cause of siderosis is retained IOFB containing iron or an iron alloy. By mechanism of injury, hammer-and-chisel work is the most common, and metal fragments during metalworking or construction are the most common source of injury.1)
The patients are 96.49% male, and the condition is strongly associated with occupational metal work.1)
The cause of chalcosis is retained IOFB containing copper or a copper alloy. Work in factories or foundries, injury to agricultural machinery, and detonator explosions are among the reported mechanisms of injury.
The diagnosis of siderosis and chalcosis is made by confirming the presence and location of an IOFB and assessing metal toxicity in the eye tissues. In missed IOFB cases, the history of injury may be unclear, so it is important to note that they are often mistaken for other diseases.3)
Detection of iron IOFBs: CT is useful for locating metallic IOFBs and can be key to diagnosis even in missed cases2).
Preventing misses: Even when the history is unclear, a systematic CT search can find an IOFB.
Detection of copper IOFB: Copper and copper alloys can also be detected as metal, but be careful about artifacts.
Ultrasound examination
Noninvasive intraocular evaluation: Highly useful in cases where fundus observation is difficult (lens opacity, vitreous hemorrhage).
Localization of the IOFB: useful for narrowing down the site, such as the vitreous cavity or subretinal space.
Electroretinography (ERG)
b-wave attenuation: As an indicator of rod function, it detects early changes. It is the most important factor for deciding the timing of treatment for siderosis. 4)
Severity assessment: Changes in the electroretinogram pattern reflect the degree of progression of iron toxicity.
Slit-lamp microscopy and OCT
Characteristic findings of chalcosis: A slit lamp is essential to confirm an emerald ring or Kayser-Fleischer ring–like changes.
OCT: Quantitatively evaluates the degree of degeneration in the RPE and photoreceptor layers, and is also used for postoperative follow-up.
In chalcosis, the Kayser-Fleischer ring is similar to that seen in Wilson disease (hepatolenticular degeneration), so differential diagnosis is needed in cases with an unclear history of trauma. Wilson disease is accompanied by systemic abnormalities of copper metabolism (decreased serum ceruloplasmin and increased urinary copper excretion), whereas chalcosis is limited to local copper deposition. Perform copper metabolism tests as needed.
In missed IOFB cases with a chronic course, this may be misdiagnosed as chronic anterior uveitis.3) In refractory uveitis or unexplained lens opacity and iris discoloration, it is important to ask about trauma history in detail and actively look for IOFB with CT imaging.
The visual acuity distribution at presentation in the 58-eye cohort by Parameswarappa et al. (2023) is shown below.1)
Visual acuity
Proportion
0.5 or higher (good)
About 34%
0.1–0.4 (moderate reduction)
About 29%
Below 0.1 (severe reduction)
About 37%
QCan siderosis be ruled out if a foreign body is not found on CT?
A
CT sensitivity depends on the size, material, and scan conditions. It is useful for metallic IOFBs, but very small or nonmetallic foreign bodies may not be detected on CT2). A comprehensive judgment that also considers clinical findings (such as iron-induced mydriasis and siderotic cataract) is needed.
Use of a magnetic probe: A magnetic probe is effective for iron-containing IOFBs and is used together with PPV to remove the foreign body from the eye.3)
Combined cataract surgery: If lens opacity (siderotic cataract) is present, combined PPV and cataract surgery may be considered depending on the case2).
IOFB removal group vs non-removal group: The removal group had a mean logMAR of 1.0, while the non-removal group had a mean logMAR of 1.58, showing significantly better visual outcomes in the removal group.1)
Copper is nonmagnetic, so removal with an electromagnet is impossible, and PPV is required.
Acute type (pure copper): Emergency surgery is needed. Perform IOFB removal by PPV and anti-inflammatory treatment equivalent to that for endophthalmitis (steroid administration). There is a high risk of progressing to ocular atrophy.
Chronic type (brass, copper alloy): Early PPV + foreign body removal. Use steroids to control postoperative inflammation.
If siderotic glaucoma develops, intraocular pressure must be controlled with eye drops, oral medication, or surgery4). Long-term intraocular pressure monitoring remains important even after foreign body removal.
QWhat happens if an IOFB is left in place for a long time?
A
Iron toxicity is persistent and progressive, and if left untreated, vision loss, night blindness, and visual field narrowing progress irreversibly4). Long-term follow-up is also needed after foreign body removal. In the pure copper form of chalcosis, there is also a risk of acute atrophy of the eyeball.
Iron remaining inside the eye gradually oxidizes and dissolves, and spreads through ocular tissues as iron ions (Fe²⁺/Fe³⁺). The central mechanisms of cell damage caused by iron ions are the following two reaction pathways.4, 3)
Haber-Weiss reaction and Fenton reaction: Iron ions catalyze the generation of reactive oxygen species (ROS), especially hydroxyl radicals (·OH). Hydroxyl radicals cause lipid peroxidation of cell membranes, DNA damage, and protein denaturation.
In ocular siderosis, rods are damaged before cones. On electroretinography, the dark-adapted b-wave (rod-derived) is the first to be reduced, followed with progression by loss of the a-wave and eventually complete disappearance of the electroretinogram.4) This rod selectivity is due to the cGMP phosphodiesterase in the rod outer segments being especially sensitive to oxidative stress caused by iron ions.
Iron deposits in the trabecular meshwork cause mechanical blockage of the outflow pathway and cytotoxicity. 4) This increases resistance to aqueous humor outflow and leads to secondary open-angle glaucoma. Even after the foreign body is removed, trabecular meshwork damage may persist, requiring long-term intraocular pressure control.
The toxic effects of copper ions depend on the copper concentration.
High-concentration copper (pure copper ≥90%): Copper ions cause acute cell membrane destruction and protein denaturation, leading to a severe inflammatory reaction like endophthalmitis. Direct injury to the vitreous, retina, and cornea progresses rapidly and may lead to phthisis bulbi.
Low-concentration copper (brass/copper alloy): Copper ions are deposited chronically in ocular tissues. Deposits in Descemet’s membrane of the cornea form Kayser-Fleischer ring-like changes, and deposits on the anterior lens capsule form an emerald ring. In the retina, a metallic yellow reflex appears.
In Wilson disease, systemic copper deposition occurs because of a systemic copper metabolism disorder (impaired ceruloplasmin production), whereas in ocular chalcosis the pathology differs because of tissue damage caused by copper released locally from an IOFB.
7. Latest research and future prospects (reports at the research stage)
Functional assessment with electroretinography is being studied as an important indicator for deciding surgical indications in ocular siderosis. By quantifying the correlation between the degree of b-wave reduction and actual retinal tissue damage, removing the IOFB during the early window, when iron toxicity is present but irreversible damage has not yet occurred, may help preserve vision. 4)
Some reports have observed improvement in electroretinogram findings (about 40% partial recovery) when the IOFB is removed early. When iron-ion-induced oxidative stress is still mild, tissue function may recover after removal, supporting early intervention.
A key challenge is standardizing a system for ongoing regular assessment of intraocular pressure, visual fields, and the optic nerve so that delayed rises in eye pressure and declines in retinal function are not missed.
Improved detection accuracy for tiny IOFBs with high-resolution CT, along with advances in MRI safety assessment techniques, may make preoperative evaluation of iron and copper foreign bodies more precise. In particular, deciding whether MRI is appropriate for foreign bodies with mixed compositions, such as copper alloys, is an important research topic.
Parameswarappa DC, Das AV, Venugopal R, Karad M, Tyagi M. Clinical profile, demographic distribution, and outcomes of ocular siderosis: electronic medical record-driven big data analytics from an eye care network in India. Indian J Ophthalmol. 2023;71(2):418-423. doi:10.4103/ijo.IJO_1446_22.
Chuah Gim Seah S, Muhammed J, Annie L, Othman K. Missed intraocular foreign body presenting as siderosis bulbi: two case reports. Cureus. 2024;16(2):e53839. doi:10.7759/cureus.53839.
Chai Y, Yeak J, Palikat J. The Rusty Eye: Ocular Siderosis Masquerading as Chronic Anterior Uveitis. Cureus. 2026;18(1):e101280. doi:10.7759/cureus.101280.
Kannan NB, Adenuga OO, Rajan RP, Ramasamy K. Management of ocular siderosis: visual outcome and electroretinographic changes. J Ophthalmol. 2016;2016:7272465. doi:10.1155/2016/7272465.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.