Wilson disease is a disorder caused by abnormalities in the copper transport membrane protein ATP7B in the liver, leading to impaired biliary copper excretion and secretion of ceruloplasmin into the blood, resulting in copper accumulation in various organs. It is also called hepatolenticular degeneration.
The Kayser-Fleischer (KF) ring is a copper deposit in the peripheral cornea at the level of Descemet’s membrane. It is 1–3 mm wide, usually brown, but may appear yellow or green 1). It first appears in the superior and inferior cornea, then extends circumferentially. There is no clear zone between the ring and the limbus.
KF rings are present in 60–90% of Wilson disease patients. They are found in 59% of asymptomatic cases but in nearly 100% of those with neurological symptoms 2). The KF ring is useful for diagnosis but is not a mandatory finding.
QCan KF rings occur in conditions other than Wilson disease?
A
When copper or copper alloy is present as an intraocular foreign body, a yellowish-green ring similar to the KF ring may appear near the corneal limbus (corneal chalcosis). It can also occur in hypercupremia. However, KF rings due to systemic copper metabolism disorders are considered unique to Wilson disease and are useful for screening and early detection. Fleischer rings in keratoconus are due to iron deposition and are a different finding.
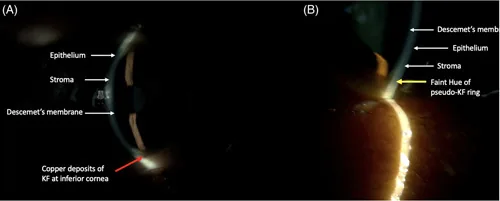
Sabhapandit S, et al. Presence of pseudo-Kayser-Fleischer rings in patients without Wilson disease: a prospective cohort study. Hepatology Communications. 2023;7(5):e0136. Figure 3. PMCID: PMC10109461. License: CC BY.
A shows copper deposition in Kayser-Fleischer ring, B shows the color difference of pseudo-Kayser-Fleischer ring for differential diagnosis. A peripheral corneal deposition ring is a clue to Wilson disease.
Slit-lamp microscopy: Brown to yellow-green annular deposits at the level of Descemet’s membrane, encircling the entire peripheral cornea1). Observed as deposits at the corneal endothelial level under parallelepiped illumination 1).
Detection in early cases: In early stages, Kayser-Fleischer rings may be incomplete and difficult to detect with slit-lamp alone; gonioscopy may be necessary.
Sunflower Cataract
Copper deposition on the anterior lens capsule: Copper may also deposit on the anterior lens capsule, known as sunflower cataract.
Other ocular motor disorders: Slowing of saccades, upward gaze palsy, and strabismus have been reported 4).
With treatment, Kayser-Fleischer rings may diminish or disappear. Resolution proceeds in the reverse order of appearance (from full circumference to only superior and inferior portions, then disappearance).
In a 19-year-old woman who started D-penicillamine therapy, marked fading of Kayser-Fleischer rings was observed within as short as 6 months 2). Although resolution of Kayser-Fleischer rings usually takes several years, rapid resolution as in this case has also been reported 2). Resolution has also been confirmed after liver transplantation, but the speed varies among cases 2).
QWhat clinical picture should raise suspicion for Wilson disease?
A
Typical suspicious symptoms include unexplained liver disease (chronic hepatitis, cirrhosis) in young individuals, unexplained extrapyramidal symptoms (tremor, dystonia), and psychiatric symptoms. Atypical presentations such as renal symptoms (cases presenting as IgA nephropathy have been reported 4)) or hematological abnormalities (cases discovered as giant platelet disorder 3)) also require consideration of Wilson disease in the differential diagnosis. Detection of Kayser-Fleischer rings on slit-lamp examination provides strong support for the diagnosis.
Wilson disease is an autosomal recessive disorder caused by mutations in the ATP7B gene (chromosome 13). ATP7B is involved in copper transport in hepatocytes, mediating biliary copper excretion and copper incorporation into ceruloplasmin. Loss of ATP7B function impairs copper excretion, leading to copper accumulation in the liver and other organs throughout the body.
Marked phenotypic discordance has been reported in monozygotic twins with identical ATP7B mutations: one twin developed severe neurological symptoms (wheelchair-bound, mutism) with positive Kayser-Fleischer rings, while the other was asymptomatic with only mild liver enzyme elevation 5). The degree of Kayser-Fleischer ring expression may also differ between twins 5). Epigenetic mechanisms (lifestyle, pregnancy, methionine metabolism, DNA methylation) are hypothesized to contribute to phenotypic discordance 5).
Wilson disease is a genetic disorder; no environmental risk factors have been identified. As an autosomal recessive condition, there is a 25% chance of developing the disease if both parents are carriers.
The Leipzig score is used for the diagnosis of Wilson disease. The presence of Kayser-Fleischer rings is worth 2 points and is an important diagnostic element 3).
The mainstay of treatment is decoppering with oral copper chelators or zinc therapy. Lifelong treatment is necessary.
Copper chelating agents
D-penicillamine (Metalcaptase®): First-line drug. It binds copper and promotes urinary excretion. Long-term oral administration may cause Kayser-Fleischer rings to disappear. Side effects include nephropathy (nephrotic syndrome), bone marrow suppression, and skin rash.
Trientine (Metalite®): An alternative drug used when side effects of D-penicillamine occur. Trientine tetrahydrochloride (Cuprior®) has recently become available 1).
Zinc agents
Zinc preparations: They inhibit copper absorption in the gastrointestinal tract. Used in combination with chelating agents or alone.
Precautions: Long-term zinc monotherapy may cause copper deficiency 7). Copper deficiency can lead to pancytopenia and spinal cord posterior column disease (myelopathy) 7). During long-term treatment, regular blood counts and serum copper monitoring are necessary 7).
Liver transplantation is indicated for fulminant hepatic failure. It has been confirmed that Kayser-Fleischer rings disappear after liver transplantation 2).
During treatment, regular monitoring of liver enzymes, INR, complete blood count, urinalysis, serum copper, and ceruloplasmin is recommended. Measure 24-hour urinary copper excretion once a year.
QDo Kayser-Fleischer rings disappear with treatment?
A
Treatment with copper chelators (D-penicillamine, trientine) can reduce or resolve Kayser-Fleischer rings. Regression occurs in the reverse order of appearance and usually takes several years. However, rapid regression within 6 months has been reported in a 19-year-old woman treated with D-penicillamine 2). Disappearance has also been confirmed after liver transplantation. It should be noted that regression of Kayser-Fleischer rings does not necessarily correlate with improvement in systemic symptoms 2).
Normally, ATP7B binds copper to ceruloplasmin within hepatocytes and secretes it into the blood, while also excreting excess copper into bile. Loss of ATP7B function reduces biliary copper excretion and impairs copper binding to ceruloplasmin. As a result, non-ceruloplasmin-bound copper (free copper) increases, and copper accumulates in the liver, brain (putamen), cornea, kidneys, and other organs.
Free copper in the aqueous humor, loosely bound to albumin, deposits in Descemet’s membrane 2). Copper deposition is limited to the depth of Descemet’s membrane, forming a ring-shaped lesion 1–3 mm wide. The absence of a clear zone between the ring and the limbus is an important distinguishing feature from arcus senilis. Deposition first appears in the superior and inferior cornea, then extends circumferentially.
Copper exerts tissue toxicity through radical production. In the liver, production of reactive oxygen species (ROS) via the Fenton reaction causes hepatocyte damage. In the brain, copper accumulation in the basal ganglia (especially the putamen) leads to extrapyramidal symptoms.
Copper accumulation in leukocytes can cause swelling of intracellular mitochondria and formation of inclusion body-like structures 3). A report using mass spectrometry found that copper concentration in leukocytes was approximately 20 times that of controls, drawing attention as a new indicator of copper toxicity 3).
Wilson disease can present with various organ disorders beyond typical hepatic and neurological symptoms. In a 26-year-old man with IgA nephropathy as the initial symptom, unexplained liver dysfunction and mild finger tremor led to suspicion of the disease, and Kayser-Fleischer rings were confirmed by slit-lamp examination, leading to a definitive diagnosis 4).
In a 48-year-old woman, giant platelets and leukocyte inclusion bodies were the initial findings. When neurological symptoms appeared two years later, Kayser-Fleischer rings were discovered on slit-lamp examination, and Wilson disease was diagnosed with a Leipzig score of 4 (Kayser-Fleischer rings 2 points, neurological symptoms 1 point, genetic mutation 1 point) 3).
In monozygotic twins with the same ATP7B mutation (c.2304dupC + c.3207C>A/His1069Gln), a marked phenotypic difference was reported: one had severe neurological type (wheelchair-bound, mutism, positive Kayser-Fleischer rings), while the other was almost asymptomatic (only mild liver enzyme elevation)5). The severe case showed dramatic neurological improvement with high-dose D-penicillamine (up to 1800 mg/day) and subsequent switch to Cuprior®5).
Challenges in Diagnosis and Management of Pediatric Wilson Disease
In childhood Wilson disease, clinical symptoms are nonspecific, leading to delayed diagnosis6). Low ceruloplasmin has high sensitivity but limited specificity because it also decreases in acute hepatitis and nephrotic syndrome6). Genetic testing is playing an increasingly important role6).
Among 338 patients receiving long-term zinc therapy, iatrogenic copper deficiency occurred in 3 cases (median duration >16 years)7). Copper deficiency causes pancytopenia (especially neutropenia) and spinal posterior column disease; cytopenia recovers with treatment adjustment, but neurological symptoms improve only partially7). Copper deficiency optic neuropathy progresses slowly and can lead to irreversible visual impairment if untreated7).
Just MD, Chang J, Herwig-Carl MC. Kayser-Fleischer Corneal Ring in Wilson’s Disease. Deutsches Arzteblatt international. 2024;121(16):544. doi:10.3238/arztebl.m2024.0048. PMID:39411902; PMCID:PMC11542566.
Sethi M, Madan S, Beri S. Fading Kayser-Fleischer ring revisited. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2021;35(2):146-148. doi:10.4103/1319-4534.337854. PMID:35391817; PMCID:PMC8982938.
Lin S, Cai J, Huang Y, et al. Macrothrombocytopenia with leukocyte inclusions in a patient with Wilson disease: a case report and literature review. BMC Med Genomics. 2024;17(1):160.
Zhang Y, Jian G, He P, et al. Immunoglobulin A nephropathy as the first clinical presentation of Wilson disease: a case report and literature review. BMC Gastroenterol. 2021;21(1):399.
Samadzadeh S, Kruschel T, Novak M, Kallenbach M, Hefter H. Different Response Behavior to Therapeutic Approaches in Homozygotic Wilson’s Disease Twins with Clinical Phenotypic Variability: Case Report and Literature Review. Genes. 2022;13(7). doi:10.3390/genes13071217. PMID:35885998; PMCID:PMC9318625.
Ungureanu IM, Iesanu MI, Boboc C, Cosoreanu V, Vatra L, Kadar A, et al. Addressing the Challenges in the Diagnosis and Management of Pediatric Wilson’s Disease-Case Report and Literature Review. Medicina (Kaunas, Lithuania). 2023;59(4). doi:10.3390/medicina59040786. PMID:37109744; PMCID:PMC10144359.
Chevalier K, Obadia MA, Djebrani-Oussedik N, Poujois A. Can patients with Wilson’s disease develop copper deficiency? Mov Disord Clin Pract. 2023;10(12):1791-1800.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.