Goldenhar syndrome
Accessory auricle and preauricular fistula: Accompanied by ear abnormalities.
Spinal abnormalities: Associated with vertebral malformations.
Mandibular hypoplasia: Causes facial asymmetry.

Lipodermoid, also called dermolipoma, is a congenital choristoma of the ocular surface containing adipose tissue. A choristoma refers to histologically normal tissue present in an abnormal location and is not a true tumor. It is thought to form from ectodermal tissue trapped within the mesoderm during optic cup formation.
Dermoid is a general term for choristomas arising in the cornea, limbus, or conjunctiva, resulting from abnormal development of the first and second branchial arches during embryogenesis. Lipodermoid is a similar choristoma but is characterized by containing more fatty components. It is non-hereditary, sporadic, and unilateral from birth.
Choristomatous lesions account for 10–30% of conjunctival tumors in children, and epibulbar dermoids are the most common episcleral choristomas in children 1). The median age at presentation is 16 years, with a female predominance.
There is a strong association with Goldenhar syndrome; 32% of 57 Goldenhar syndrome cases had epibulbar dermoids or lipodermoids. Conversely, in a case series of lipodermoids, 35% had Goldenhar syndrome.
Dermolipoma is a choristoma, in which normal tissue is present in an ectopic location. It has no potential for malignancy and follows a benign course.
Dermolipoma is congenital, but often remains asymptomatic for many years and may not be discovered until adulthood. It is often first noticed when lifting the eyelid for makeup application or contact lens insertion.
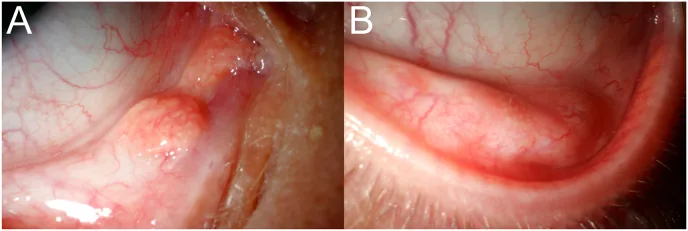
Dermolipoma appears as a yellowish-white, firm mass adherent to the conjunctiva. It cannot be moved freely and cannot be repositioned into the orbit. It is usually unilateral but can be bilateral.
The main clinical signs are shown below.
| Sign | Characteristic |
|---|---|
| Yellow-white mass | Hard, palpable |
| Distortion of the lateral canthus | Deformity due to mass |
| Astigmatism | Due to corneal deformation |
| Strabismus | Rarely associated |
Astigmatism induced by dermolipoma itself is milder than that caused by dermoid. However, if corneal astigmatism is present, there is a risk of amblyopia, and regular evaluation with visual acuity and refraction tests is important.
Dermolipoma is a congenital choristoma derived from ectodermal sequestration during embryonic development. Abnormalities in the formation of the first and second branchial arches during the embryonic period are involved.
It may occur in isolation, but it can also occur in association with the following systemic syndromes.
Goldenhar syndrome
Accessory auricle and preauricular fistula: Accompanied by ear abnormalities.
Spinal abnormalities: Associated with vertebral malformations.
Mandibular hypoplasia: Causes facial asymmetry.
Other related syndromes
Other associations include coloboma, osteoma, corneal limbal dermoid, and facial nerve palsy.
A systemic examination is necessary to check for ear abnormalities such as accessory ear and preauricular fistula, spinal deformities, and mandibular hypoplasia. For details, refer to the “Causes and Risk Factors” section.
Dermolipoma is located near the surface, so it can be easily diagnosed by clinical examination.
On CT/MRI, it appears as a crescent-shaped or triangular fatty mass anterior to the insertion of the lateral rectus muscle in the superotemporal quadrant of the globe and medial to the lacrimal gland. Usually, there is no continuity with intraconal fat. Since it is a benign lesion, CT exposure should be avoided as much as possible, especially in children.
| Differential diagnosis | Key points for differentiation |
|---|---|
| Orbital fat prolapse | Common in elderly. Increases with pressure |
| Dermoid cyst | Cystic. Retains secretions |
| Lacrimal gland cyst/prolapse | Localized to lacrimal gland area |
| Conjunctival lymphangioma | Salmon pink color |
| Conjunctival lymphoma | Salmon pink color. Elderly patients |
It consists of adipose tissue, collagen tissue, and skin appendages (which may include hair follicle sebaceous structures and lacrimal gland tissue), and is covered by connective tissue and the surface epithelium of the conjunctiva. As it is a choristoma, it is composed of normal tissue and has no potential for malignant transformation.
Small, asymptomatic dermolipomas do not require treatment. Symptoms may be managed with lubrication using artificial tears or anti-inflammatory eye drops.
Surgery is considered in the following cases.
Rather than complete resection, surgical debulking is the standard approach. Only the anterior portion of the mass is removed, preserving the conjunctiva while removing as much of the dermolipoma and pilosebaceous units anterior to the orbital rim as possible.
Simple excision of a limbal dermoid alone often leads to recurrence and pseudopterygium, and because it extends into the corneal stroma, the cornea becomes thin after excision. Therefore, combined superficial keratoplasty is recommended.
If the lesion is small and asymptomatic, surgery is not required, and conservative treatment such as artificial tears may be sufficient. Surgical indications are limited to cases with visual axis involvement, induced astigmatism, persistent irritation, or cosmetic concerns. For details, see the section on “Standard Treatment.”
A choristoma is a mass of histologically normal tissue located in an abnormal site. In contrast, a hamartoma is a benign tumor composed of an abnormal mixture of cells and tissues normally present at that site; the two are conceptually distinct.
The tissues composing a dermolipoma include both ectodermal derivatives (hair, skin, and rarely teeth) and mesodermal derivatives (adipose tissue, cartilage). It may also adhere to the lacrimal gland or underlying bone.
Dermolipoma
Adipose tissue: Contains a large amount and is the main component.
Epithelium: Covered by surface epithelium continuous with the conjunctiva.
Adnexa: May include pilosebaceous structures and lacrimal gland tissue.
Dermoid
Connective tissue: Mainly composed of collagen connective tissue resembling the dermis.
Epithelium: Composed of epidermal epithelium.
Interior: Filled with collagen fibers, including sebaceous glands, hair follicles, and sweat glands.
Both are separation tumors, thus composed of normal tissue, with no potential for malignancy.
Conventional excision of limbal dermoid has been associated with recurrence and pseudopterygium formation after simple excision. Recently, the usefulness of lamellar corneal patch grafts for surface reconstruction after excision has been reported.
Roels (2024) performed lamellar corneoscleral excision followed by anterior lamellar corneal patch graft transplantation in three cases of limbal dermoid (4-year-old, 18-year-old, and 8-year-old, all female). Pathological examination confirmed benign lipodermoid in all cases. Corneal astigmatism decreased from 2.75 D to 0.75 D in case 1 and stabilized at 1.75 D in case 2. Case 3 had preexisting severe amblyopia, and surgery was performed for cosmetic purposes only. In all cases, the postoperative corneal graft was clear with no inflammation or epithelial defects, and no recurrence or pterygium formation was observed during follow-up1).
This report indicates that the depth, size, and location of the lesion are important factors in surgical planning and suggests that combining corneal patch grafts may achieve excellent anatomical and visual outcomes1).