
Laser flare meter (measurement of anterior chamber protein concentration and inflammation evaluation) (Laser Flare Meter)
Key points at a glance
Section titled “Key points at a glance”What is a laser flare meter?
Section titled “What is a laser flare meter?”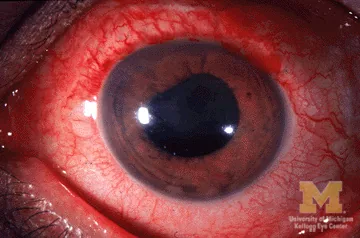
A laser flare meter directs a He-Ne laser beam into the anterior chamber and electronically measures the Tyndall phenomenon (light scattering) caused by protein in the aqueous humor. It can objectively quantify anterior chamber protein concentration in photon count/ms (ph/ms).
Anterior chamber flare is an indicator that reflects protein concentration in the anterior chamber. There are two main mechanisms for an increase in flare. First, inflammation or neovascularization disrupts the blood-aqueous barrier of the iris and ciliary body, allowing plasma proteins to leak into the anterior chamber. Second, reduced ciliary body function worsens aqueous humor circulation, causing waste proteins to accumulate in the anterior chamber.
Subjective grading using a slit-lamp microscope is an essential skill in daily practice. However, subjective assessment leads to interfacility and interobserver variability. The laser flare meter complements this limitation and enables quantitative tracking of inflammation over time.
The SUN Working Group (Standardization of Uveitis Nomenclature) has established international standard grading criteria for anterior chamber flare and anterior chamber cells, and these have been adopted in uveitis treatment guidelines1)2).
The protein concentration in the anterior chamber can be objectively quantified in ph/ms (photon count/ms). It can be used to track uveitis inflammatory activity and treatment response numerically, and it can also evaluate the course of inflammatory reaction after cataract surgery. A key feature is that it can detect subtle, low-grade changes that are difficult to see with a slit-lamp microscope.
2. Examination method
Section titled “2. Examination method”Measurement with a laser flare meter
Section titled “Measurement with a laser flare meter”A representative device is the KOWA FM-600 (successor to the FM-500). He-Ne laser light (wavelength 675 nm) is directed into the anterior chamber, and the scattered light is received by a photomultiplier (photomultiplier tube) and converted into photon count.
- Measurement unit: photon count/ms (ph/ms)
- Adult normal value: 3–7 ph/ms (varies by device and individual)
- Measurement method: Non-contact, non-invasive. Pupil dilation is not required. One measurement takes just a few seconds.
- Standard protocol: Measure 7 times and use the average of the 5 measurements after excluding the highest and lowest values
- Measurement accuracy: the actual measured value after subtracting background noise is taken as the anterior chamber flare value
Flare grading by slit-lamp microscopy (SUN criteria)
Section titled “Flare grading by slit-lamp microscopy (SUN criteria)”Narrow the slit width and set the height to about 3 mm, then shine the light at an angle that makes the beam width visible in the anterior chamber and observe it from the front. When protein concentration in the anterior chamber increases, the light path that is usually not visible becomes clearly seen through the Tyndall phenomenon.
The SUN Working Group grading criteria for anterior chamber flare are as follows1)2).
| Grade | Description |
|---|---|
| 0 | none (none) |
| 1+ | faint (mild) |
| 2+ | moderate (moderate) The details of the iris and lens are clear |
| 3+ | marked (severe) details of the iris and lens are indistinct |
| 4+ | intense (marked) fibrin or plastic aqueous humor |
The SUN Working Group grading criteria for anterior chamber cells (number of cells per one 1×1 mm slit-lamp field) are as follows1)2).
| Grade | Number of cells seen in one field |
|---|---|
| 0 | <1 (fewer than 1) |
| 0.5+ | 1–5 |
| 1+ | 6–15 |
| 2+ | 16〜25 |
| 3+ | 26〜50 |
| 4+ | >50 (51 or more) |
(1 field of view = the field of the 1 × 1 mm slit beam of the slit-lamp microscope)
Flare grading with a slit-lamp microscope is a subjective five-step evaluation from 0 to 4+ according to the SUN criteria. It is prone to variability between facilities and observers. The laser flare meter provides an objective quantitative value in ph/ms, making it useful for detecting subtle changes in low-grade inflammation and for longitudinal follow-up. In daily practice, slit-lamp grading is standard, while the flare meter is used when quantitative evaluation is needed.
3. Evaluation system for anterior chamber inflammatory findings
Section titled “3. Evaluation system for anterior chamber inflammatory findings”Evaluation of anterior chamber inflammation is done by systematically observing flare, cells, aqueous convection, hypopyon, and fibrin.
- Anterior chamber flare: reflects an increase in protein concentration in the anterior chamber. It is caused by two mechanisms: breakdown of the vascular barrier (inflammation, neovascularization) and decreased ciliary body function
- Anterior chamber cells: Count the number of inflammatory cells in one 1×1 mm slit-lamp field according to the SUN criteria. Neutrophils, lymphocytes, and plasma cells may be mixed together1)
- Aqueous flare: Observe this together with cell grading. It reflects aqueous humor production and the protein concentration in the anterior chamber, and is useful for judging disease activity and treatment response
- Hypopyon: Seen as white deposits in the lower anterior chamber. It is divided into a loose type that moves with changes in posture and a clumped type that remains fixed
The two types of hypopyon are shown below.
| Classification | Features | Representative disease |
|---|---|---|
| Loose type | Changes with posture | Acute Behçet disease, severe bacterial endophthalmitis |
| Clumped fixed type | Fixed in one location | Inflammation with mononuclear cells and fibrin deposition |
The most severe form of flare: fibrin in the anterior chamber
Section titled “The most severe form of flare: fibrin in the anterior chamber”Anterior chamber fibrin is the most severe form of flare. It is observed as a distinct clot, or as hazy, cotton-like precipitates, in the anterior chamber. Fibrin deposition often causes posterior synechiae (posterior iris synechiae) and elevated intraocular pressure, so special caution is needed.
Definition of inflammatory activity according to SUN criteria
Section titled “Definition of inflammatory activity according to SUN criteria”According to SUN Working Group criteria, uveitis activity is defined as follows2).
- inactive: grade 0
- worsening: an increase of 2 grades or more
- improved: a decrease of 2 grades or more
- remission: inactivity lasting 3 months or longer without medication
Clinical significance and indications
Section titled “Clinical significance and indications”Monitoring uveitis activity
Section titled “Monitoring uveitis activity”Laser Flare Meter is a recommended method for quantifying anterior chamber flare in uveitis clinical practice guidelines1). It correlates well with slit-lamp findings and is useful for quantitatively tracking the course of treatment. It is especially valuable in the following situations.
- Detection of subtle inflammatory changes in low-activity uveitis
- Quantitative assessment of treatment effects of immunosuppressants and biologic agents
- Outcome measures in clinical research
The most common diseases in uveitis are sarcoidosis (10.7%), VKH disease (Vogt-Koyanagi-Harada disease, 7.0%), and acute anterior uveitis (6.6%)1). These diseases require long-term inflammation monitoring, and quantitative flare meter assessment is useful for adjusting treatment.
Assessment of post-cataract surgery inflammation
Section titled “Assessment of post-cataract surgery inflammation”The speed at which the postoperative anterior chamber flare value returns to normal is a measure of postoperative management. After cataract surgery, it generally begins to decrease gradually from 1 week after surgery, and recovery to the normal range (3–7 ph/ms) is expected within 1 to 3 months after surgery3). Persistently elevated flare values suggest prolonged postoperative inflammation or complications such as cystoid macular edema.
Assessment of biologic therapy effects
Section titled “Assessment of biologic therapy effects”In the treatment of uveitis with biologic agents such as adalimumab and infliximab, flare meter values are used as biomarkers of treatment response4). They can detect flare-ups and improvement in inflammation more sensitively than slit-lamp grading.
Relationship with keratic precipitates (KP)
Section titled “Relationship with keratic precipitates (KP)”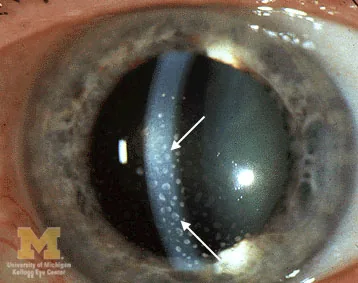
KP (keratic precipitates, deposits on the posterior corneal surface) are deposits and clusters of white blood cells, iris pigment, and red blood cells in the aqueous humor on the back surface of the cornea. The characteristics and distribution of KP, when combined with flare findings, help support disease differentiation.
The characteristics of KP and the related diseases are shown below.
| KP type | Characteristics | Suspected disease |
|---|---|---|
| Mutton-fat KP | Large, fatty appearance | Sarcoidosis, VKH disease (granulomatous uveitis) |
| Fine KP | Small, fine | Non-granulomatous uveitis |
| White KP | Indicates fresh, active inflammation | Current active intraocular inflammation |
| Brown KP | Old KP with iris pigment | Residual past inflammation (inactive) |
The distribution of KP is also a clue for diagnosis. They are usually seen more often in the triangular area below the center of the cornea because of aqueous humor convection. If small white scattered KPs are seen as far up as the upper part, Fuchs heterochromic iridocyclitis (Fuchs iritis syndrome) is suspected. KP with a stellate appearance are characteristically seen in infectious uveitis such as herpetic iritis.
It is especially useful in the following three situations: 1) Long-term follow-up of low-activity uveitis: subtle inflammatory changes that are difficult to detect with slit-lamp grading can be captured as changes in ph/ms values. 2) Evaluation of post-cataract surgery inflammation: the speed at which the flare value returns to normal can objectively show how postoperative inflammation is settling. 3) Outcome assessment in clinical research: used as a standard quantitative outcome measure in clinical trials of uveitis treatments.
5. Interpretation and management of test results
Section titled “5. Interpretation and management of test results”The following are general guidelines for interpreting laser flare meter values.
- Normal range (3–7 ph/ms): Reference values for healthy adults. There are device and individual differences
- Mild elevation (about 8–15 ph/ms): May be within the acceptable range as low-grade inflammation or an early physiological response after surgery
- Moderate elevation (about 15–50 ph/ms): Active anterior uveitis or prolonged postoperative inflammation is suspected. Consider strengthening steroid eye drops
- Marked elevation (50 ph/ms or more): Severe inflammation. Risk of fibrin deposition, posterior synechiae, and increased intraocular pressure is high. Use steroid eye drops such as fluorometholone at high frequency (e.g., every hour) and use 0.5–1% atropine sulfate eye drops to dilate the pupil and paralyze the ciliary muscle
The correlation coefficient between the flare value in uveitis and slit-lamp grading is said to be about 0.6–0.8. As the grade increases, the ph/ms value also increases, but because individual variation is large, tracking each patient’s changes over time is more important than comparing absolute values5).
Under the SUN criteria, treatment response is judged by a change of two or more grades2). With a flare meter, the rate of decrease in the ph/ms value within 1–2 weeks after starting treatment can be an early indicator of response3).
The basic approach to treatment depends on the underlying disease. In general, consider the following:
- Steroid eye drops: Betamethasone 0.1% eye drops, fluorometholone 0.1% eye drops, and similar. Frequent instillation 4–12 times a day depending on the severity of inflammation
- Mydriatic agents: Atropine sulfate 0.5–1% eye drops (to prevent posterior synechiae of the iris and reduce pain by paralyzing the ciliary muscle) or tropicamide 0.5% eye drops
- Oral or intravenous steroids: In severe cases, oral prednisolone (0.5–1 mg/kg/day) or high-dose intravenous methylprednisolone 500–1000 mg/day for 3 days
- Immunosuppressants: Cyclosporine, tacrolimus, methotrexate, and others are used in refractory cases
- Biologics: Adalimumab (covered by insurance for noninfectious uveitis) and infliximab, among others
6. Measurement Principle (Details of the Optical Principle)
Section titled “6. Measurement Principle (Details of the Optical Principle)”The optical principle of the laser flare meter is based on the Tyndall effect.
- He-Ne laser light (wavelength 675 nm) is directed into the anterior chamber
- Light is scattered by protein particles in the aqueous humor (Tyndall effect). In normally clear aqueous humor, scattering is minimal, but as the protein concentration increases, the Tyndall effect becomes stronger
- Scattered light is received by a photomultiplier tube and converted into photon counts
- The measured value after subtracting background noise (non-scattered light component) becomes the anterior chamber flare value (ph/ms)
- The higher the protein concentration, the greater the amount of scattered light and the higher the ph/ms value
The essential principle of the laser flare meter is the same physical phenomenon as the Tyndall phenomenon observed with a slit-lamp microscope, which electronically quantifies it. In flare observation with a slit lamp, the light path also appears white as the slit beam passes through the anterior chamber, due to the same mechanism.
When the size of protein particles is less than 1/10 of the laser wavelength, Rayleigh scattering predominates; when it is about the same size or larger, Mie scattering predominates. Proteins in the anterior chamber (molecular weight from tens of thousands to hundreds of thousands Daltons) show scattering characteristics close to the range of Mie scattering. Because scattered light intensity is almost linearly correlated with protein concentration, protein concentration can be quantitatively estimated from the ph/ms value5)6).
7. Latest Research and Future Prospects
Section titled “7. Latest Research and Future Prospects”- Quantification of anterior chamber flare by anterior segment OCT: Imaging-based quantification of light scattering in the anterior chamber using anterior segment OCT (AS-OCT) is being explored. Research is progressing as an alternative in facilities where laser flare meters are not widely available7)
- Application to evaluating the effects of biologic agents: In the treatment of noninfectious uveitis with biologic agents such as adalimumab and infliximab, flare meter values are being studied as an early indicator of treatment response4)
- Automatic flare grading from slit-lamp images by AI: Machine-learning-based automatic flare grading from slit-lamp photographs is still in the research stage. In the future, objective standardization of subjective grading is expected
- Expanded use in evaluating inflammation after dry eye and glaucoma surgery: Reports describe its use in evaluating minor anterior chamber inflammation associated with dry eye and in monitoring inflammation after trabeculectomy8)
8. References
Section titled “8. References”- 日本眼炎症学会ぶどう膜炎診療ガイドライン作成委員会. ぶどう膜炎診療ガイドライン. 日眼会誌. 2019;123(6):635-696.
- Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. American journal of ophthalmology. 2005;140(3):509-16. doi:10.1016/j.ajo.2005.03.057. PMID:16196117; PMCID:PMC8935739.
- Oshika T, Yoshimura K, Miyata N. Postsurgical inflammation after phacoemulsification and extracapsular extraction with soft or conventional intraocular lens implantation. Journal of cataract and refractive surgery. 1992;18(4):356-61. doi:10.1016/s0886-3350(13)80071-5. PMID:1501087.
- Díaz-Llopis M, Salom D, Garcia-de-Vicuña C, Cordero-Coma M, Ortega G, Ortego N, et al. Treatment of refractory uveitis with adalimumab: a prospective multicenter study of 131 patients. Ophthalmology. 2012;119(8):1575-81. doi:10.1016/j.ophtha.2012.02.018. PMID:22525047.
- Sawa M, Tsurimaki Y, Tsuru T, Shimizu H. New quantitative method to determine protein concentration and cell number in aqueous in vivo. Jpn J Ophthalmol. 1988;32(2):132-142. PMID: 3054216.
- Ladas JG, Wheeler NC, Morhun PJ, Rimmer SO, Holland GN. Laser flare-cell photometry: methodology and clinical applications. Survey of ophthalmology. 2005;50(1):27-47. doi:10.1016/j.survophthal.2004.10.004. PMID:15621076.
- Agarwal A, Ashokkumar D, Jacob S, Agarwal A, Saravanan Y. High-speed optical coherence tomography for imaging anterior chamber inflammatory reaction in uveitis: clinical correlation and grading. American journal of ophthalmology. 2009;147(3):413-416.e3. doi:10.1016/j.ajo.2008.09.024. PMID:19054493.
- Ayala M. Laser flare photometry: a useful tool for glaucoma management. J Glaucoma. 2012;21(5):343-347.