Orbital lymphangioma (orbital lymphangioma) is a lymphatic malformation formed inside the orbit. The name “lymphangioma” has long been widely used, but today it is understood as a disease entity classified as a vascular malformation, not a tumor.
Normally, lymphatic tissue is thought not to exist inside the orbit. However, because of abnormal embryonic development, ectopic lymphatic vessels can form within the orbit. If bleeding occurs in these ectopic lymphatic vessels, the mass can rapidly enlarge and be found because of pressure symptoms such as proptosis.
Under the classification of the International Society for the Study of Vascular Anomalies (ISSVA), orbital lymphangioma is classified as a low-flow vascular malformation (lymphatic malformation)[8]. It is not a tumor and does not become malignant. The prognosis for life is good, but repeated bleeding episodes can impair visual function, so long-term management is needed[2,3].
It most often occurs in childhood (from infancy to school age), and most cases are unilateral. It is relatively rare among all orbital tumors, but it is an important condition in pediatric orbital masses[1,2]. New onset in adults is rare, but lesions that have been present since childhood can worsen in adulthood.
QIs orbital lymphangioma a tumor?
A
Strictly speaking, it is not a tumor but a vascular malformation (lymphatic malformation). It does not become malignant, and the prognosis for life is good. However, repeated bleeding inside the mass can affect vision, and in children there is also a risk of amblyopia. It is important to understand this as a chronic condition that requires long-term follow-up.
The most characteristic clinical presentation of orbital lymphangioma is sudden-onset acute eyelid swelling and proptosis. Bleeding into the lymphatic spaces (chocolate cyst formation) can cause the mass to enlarge rapidly over the course of hours [1,2].
Eyelid swelling and proptosis: rapidly enlarges during a bleeding episode
Severe eye pain: due to a sudden rise in intraorbital pressure
Nausea and vomiting: occurs when intraorbital pressure rises markedly
Globe displacement: the mass displaces the eye
Limitation of eye movements and double vision: caused by compression from the mass
Known triggers for bleeding include upper respiratory infections (the common cold, pharyngitis), trauma, and Valsalva maneuvers (straining, blowing the nose, and similar actions). In children, many cases occur after an upper respiratory infection.
Lymphatic vessels may be visible beneath the conjunctiva, and a bluish, soft mass may be felt under the eyelid skin. Some cases are accompanied by subconjunctival hemorrhage.
Acute bleeding episode
Symptoms: sudden eyelid swelling, proptosis, and severe eye pain
Course: rapid enlargement within hours
Triggers: upper respiratory infection, trauma, or Valsalva maneuver
Management: decide between conservative observation and emergency surgery depending on severity
Chronic course
Symptoms: eye deviation, eye movement disorder, and double vision
Course: gradual enlargement or stabilization
Complications: decreased vision; in children, risk of amblyopia
Management: Consider surgery or sclerotherapy if compression symptoms are severe
Rebleeding
Frequency: Rebleeding occurs in about 70% of cases during follow-up
Trigger: Upper respiratory infection is the most common
When symptoms worsen: If vision is affected or pain is severe, consider debulking surgery
Prevention: Early treatment of upper respiratory infections and avoidance of trauma
QWhy does the eye suddenly swell?
A
Swelling occurs because bleeding into the ectopic lymphatic spaces within the orbit causes a rapid increase in the size of the mass (forming a chocolate cyst). Upper respiratory infections and trauma are often triggers. Because the blood from the bleed is gradually absorbed over time, symptoms often improve on their own. However, if the amount of bleeding is large, the pressure inside the orbit can rise markedly, causing eye pain, vomiting, and decreased vision.
Orbital lymphangioma is most common in childhood (from infancy to school age) and is a relatively rare disease among all orbital tumors. However, it is an important condition in pediatric orbital masses and should always be considered in the differential diagnosis when evaluating a rapidly enlarging orbital mass in a child.
Most cases are unilateral, and bilateral cases are exceptional. Clear statistical data on sex differences are limited. New onset in adults is rare, but some cases involve lesions that began in childhood and become symptomatic in adulthood.
Rebleeding during follow-up has been reported in about 70% of cases, and repeated episodes of rebleeding over a long period may gradually impair visual function. In particular, repeated bleeding episodes in children can lead to amblyopia, so ongoing follow-up is important from the standpoint of vision management.
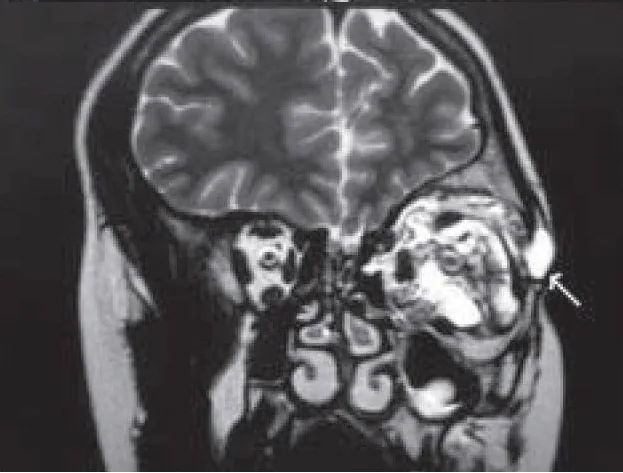
Mishra A, Alsawidi K, Abuhajar R, Ehtuish EF. Orbital venous-lymphatic malformation: Role of imaging. Oman J Ophthalmol. 2009;2(3):141-144. Figure 4B. PMCID: PMC2903921. DOI: 10.4103/0974-620X.57316. License: CC BY.
On T2-weighted coronal MRI, multiloculated cystic spaces (arrows) are seen within the orbit (intraconal). The cystic components show high T2 signal, and extension outside the cone is also confirmed. This corresponds to the MRI imaging findings of a multiloculated mass discussed in section “4. Diagnosis and examination methods.”
A cyst-like mass is seen around the eyeball. The internal appearance varies depending on the amount of bleeding. In the acute phase of bleeding, heterogeneous echoes are seen inside. Because it is noninvasive and can be performed quickly, it is useful for initial assessment in the acute phase.
It typically appears as a multilocular orbital mass. The most important diagnostic finding is fluid-fluid level [4].
Fluid-fluid level: a mirror-like layering caused by settled blood within the mass. On T2-weighted images, a low-signal sediment layer and a high-signal supernatant layer are seen. This is an important diagnostic finding of this disease.
T1-weighted images: signal intensity changes depending on the stage of bleeding. Subacute hemorrhage (methemoglobin) shows high signal.
T2-weighted images: the cystic components show high signal. The multiloculated structure is clearly depicted.
Contrast enhancement: The lymphangioma itself does not enhance (because it is a malformation without blood flow). This helps distinguish it from cavernous hemangioma (marked delayed enhancement).
It appears as an irregular low-attenuation area. During acute bleeding, it may include high-attenuation areas. It is also useful for assessing whether there is bone destruction (usually there is none).
cyst and fatty components limited to the bony margin
often occurs at bony sutures and contains fatty components
Orbital rhabdomyosarcoma grows rapidly as a solid mass and often causes bone destruction. If it is difficult to distinguish it from lymphangioma on imaging, a biopsy is needed.
QHow is it distinguished from rhabdomyosarcoma?
A
Orbital rhabdomyosarcoma is a malignant tumor that must always be ruled out in children with a rapidly enlarging orbital mass. Points that help distinguish it from lymphangioma include that rhabdomyosarcoma is a solid mass, often causes bone destruction, shows enhancement on MRI, and does not form fluid levels. If imaging alone makes it difficult to tell them apart, a biopsy is needed for histologic confirmation.
Orbital lymphangioma is not a malignant tumor, and the prognosis for life is good. The treatment plan is decided based on how severe the symptoms are, and unnecessary invasive procedures are avoided.
Conservative follow-up (for mild to moderate bleeding episodes)
If there is no indication for the emergency interventions above, bleeding in many cases resolves on its own and is gradually reabsorbed, so conservative follow-up is used. In children, follow-up with the expectation of spontaneous regression is the first choice. It is important to explain clearly to the patient and family that they should return promptly if symptoms worsen.
Conservative follow-up
Indications: Mild to moderate bleeding episodes
Rationale: Most bleeding resolves on its own and is reabsorbed
Key point: Explain that they should return promptly if symptoms worsen
Children: choose active observation, expecting spontaneous regression
Acute-phase intervention
Indications: acute enlargement with heavy bleeding and vomiting
Procedure: cooling → if there is no improvement, incision and decompression or debulking surgery
Purpose: emergency reduction of intraorbital pressure and hemostasis
Note: if there is heavy bleeding from the conjunctiva, perform debulking surgery also to stop the bleeding
Surgery and sclerotherapy in the chronic phase
Indications: chronic cases with severe pressure symptoms and facial deformity
Surgery: partial resection (debulking surgery). Complete removal is often difficult
Sclerotherapy: intracystic injection of OK-432 (Picibanil), etc. Minimally invasive and repeatable
Key point: forcing complete removal carries a risk of damage to surrounding tissues
Treatment in the acute phase (when there is major bleeding)
Treatment steps when the amount of bleeding is large and intraorbital pressure rises markedly are as follows.
Cooling: Cool the affected area in the hope of vasoconstriction and hemostasis. First tried when vomiting is severe.
If there is no improvement, incision decompression: If cooling does not sufficiently relieve intraorbital pressure, perform incision decompression.
Debulking surgery: If massive bleeding occurs from the conjunctiva, or if there is no improvement with the above measures, perform debulking surgery, which also serves to control bleeding.
Intracystic injection of OK-432 (Picibanil) has been reported as a sclerotherapy for lymphatic malformation [5]. In sclerotherapy using bleomycin, a long-term follow-up study of 69 eyes reported a good response in 79% of cases [6]. Both are positioned as minimally invasive and repeatable treatments, but the specific indications, dosage, and effectiveness require specialist evaluation for each case.
In children, repeated bleeding episodes can cause anisometropia and may lead to amblyopia. It is important to perform regular refraction and vision tests, and to provide proper vision correction and, if needed, amblyopia treatment (such as patching of the healthy eye) at the same time.
QCan it be completely removed with surgery?
A
Complete removal is often difficult. Orbital lymphangioma has poorly defined borders with the surrounding tissues, and trying to remove it completely can risk damage to the optic nerve, extraocular muscles, and eyeball. Partial removal (debulking surgery) is a realistic treatment goal for easing pressure symptoms. For cystic lesions, sclerotherapy (injection into the cyst, such as with OK-432) has been tried as a less invasive option.
QHow often does rebleeding occur?
A
It has been reported that rebleeding occurs in about 70% of cases during follow-up. Because upper respiratory infections are the most common trigger, it is important to tell patients and families to seek medical care early if they develop a cold, pharyngitis, or similar illness. If rebleeding affects vision or causes severe pain, debulking surgery should be considered.
6. Pathophysiology and detailed mechanism of onset
Orbital lymphangioma arises from an abnormality during embryonic development of the blood vessel and lymphatic systems. Normally, mature orbital tissue does not contain lymphatic tissue, but an abnormality in fetal development causes ectopic lymphatic tissue to form in the orbit. For this embryologic origin, it is classified as a malformation rather than a tumor.
Mechanism of mass enlargement (chocolate cyst formation)
Ectopic lymphatic channels have a thin-walled, multilocular cystic structure. Bleeding occurs when red blood cells seep into and accumulate within these thin-walled lymphatic spaces. As the blood components degenerate and become concentrated, a dark brown chocolate cyst forms, leading to rapid enlargement of the mass.
Potential triggers of bleeding include local inflammation caused by upper respiratory infections (congestion of the lymph nodes and blood vessels, and inflammatory responses). Trauma and increased venous pressure from Valsalva maneuvers (sneezing, blowing the nose, straining, and similar actions) can also be triggers.
Characteristics as a low-flow vascular malformation
In the ISSVA classification, a low-flow vascular malformation (lymphatic malformation) is a static malformation without blood flow. For this reason, the mass itself does not enhance on contrast studies. This feature is an important imaging clue that helps distinguish it from cavernous hemangioma (high-flow with marked delayed enhancement).
The lack of blood flow is also why treatment effects from vasoactive drugs are limited. At the same time, it is the theoretical basis for expecting benefit from sclerotherapy by directly injecting agents such as OK-432 into the cysts.
Infiltrative growth pattern and why complete removal is difficult
Orbital lymphangioma has unclear borders with the surrounding normal tissues (orbital fat, extraocular muscles, and the tissues around the optic nerve) and shows an infiltrative growth pattern. For this reason, complete surgical removal is technically difficult, and attempting to remove it carries a high risk of injuring important surrounding structures. This histologic feature is why partial removal (debulking surgery) is chosen as the practical treatment goal.
It does not become malignant and does not have the property of growing endlessly on its own. It usually follows a slow course with repeated bleeding episodes, but the main problems are effects on visual function from recurrent bleeding and amblyopia in children.
In the International Society for the Study of Vascular Anomalies (ISSVA) classification, orbital lymphangioma is clearly positioned not as a tumor but as a vascular malformation under “lymphatic malformation” [8]. With this conceptual organization, treatment strategy is also shifting from “removal” of a tumor to “symptom management and reduction” of a malformation [3].
Reports on intracystic sclerotherapy using OK-432 (Picibanil) or bleomycin are gradually accumulating [5,6]. It is attracting attention as a minimally invasive treatment that can be repeated, and reports of percutaneous sclerotherapy performed under image guidance (ultrasound-guided or CT-guided) are also increasing. However, large clinical studies focused specifically on orbital lymphangioma are still limited at present, and further validation is needed for the best indications, drug choice, concentration, and number of treatments [5].
In recent years, systemic administration of the mTOR inhibitor sirolimus has been tried for lymphatic malformations in general, and a mass-reducing effect has been reported [7]. Somatic mutations, including PIK3CA mutations, are becoming better understood as being involved in the development of lymphatic malformations at the molecular level [8], and the role of mTOR inhibitors as molecular targeted therapy may become established in the future. A systematic review of orbital lymphangioma reported partial responses in many patients treated with sirolimus, but more evidence is needed on the optimal dose, treatment duration, and long-term safety [7].
Advances in MRI technology (high-field 3.0T, various fat suppression methods, diffusion-weighted imaging, and others) now make it possible to assess the multicystic structure, fluid levels, and boundaries with surrounding tissues in greater detail. Its use as a non-invasive follow-up tool is expanding.
Tunç M, Sadri E, Char DH. Orbital lymphangioma: an analysis of 26 patients. Br J Ophthalmol. 1999;83(1):76-80. doi:10.1136/bjo.83.1.76. PMID: 10209440.
Wiegand S, Eivazi B, Bloch LM, et al. Lymphatic malformations of the orbit. Clin Exp Otorhinolaryngol. 2013;6(1):30-35. doi:10.3342/ceo.2013.6.1.30. PMID: 23526369.
Lally SE. Update on orbital lymphatic malformations. Curr Opin Ophthalmol. 2016;27(5):413-415. doi:10.1097/ICU.0000000000000291. PMID: 27219273.
Mishra A, Alsawidi K, Abuhajar R, Ehtuish EF. Orbital venous-lymphatic malformation: Role of imaging. Oman J Ophthalmol. 2009;2(3):141-144. doi:10.4103/0974-620X.57316. PMID: 20927213; PMCID: PMC2903921.
Lam SC, Yuen HKL. Medical and sclerosing agents in the treatment of orbital lymphatic malformations: what’s new? Curr Opin Ophthalmol. 2019;30(5):380-385. doi:10.1097/ICU.0000000000000585. PMID: 31232717.
Dave TV, Kavya Madhuri B, Laghmisetty S, et al. Long term outcomes of transcutaneous non-image guided bleomycin sclerotherapy in orbital/adnexal lymphatic malformations: a protocol-based management in 69 eyes. Eye (Lond). 2022;36(4):789-799. doi:10.1038/s41433-021-01527-9. PMID: 33879854.
Shoji MK, Shishido S, Freitag SK. The Use of Sirolimus for Treatment of Orbital Lymphatic Malformations: A Systematic Review. Ophthalmic Plast Reconstr Surg. 2020;36(3):215-221. doi:10.1097/IOP.0000000000001518. PMID: 31990892.
Kunimoto K, Yamamoto Y, Jinnin M. ISSVA Classification of Vascular Anomalies and Molecular Biology. Int J Mol Sci. 2022;23(4):2358. doi:10.3390/ijms23042358. PMID: 35216474.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.