An orbital dermoid cyst (orbital dermoid cyst) is a congenital choristoma caused by an abnormality in development, in which normal cells form a benign mass in a place where that tissue does not normally exist. In ICD-10, it is classified as D31.60.
There are two types of choristoma: dermoid cyst and epidermoid cyst. A dermoid cyst contains skin appendages in the cyst cavity, such as hair follicles, hair, and sebaceous glands, as well as fat and smooth muscle. An epidermoid cyst does not have appendage structures and the cavity is filled only with keratinized material from the epidermis (so-called debris). When tissues derived from the endoderm, mesoderm, and ectoderm are all present together, it is called a teratoma.
Orbital dermoid cysts account for 46% of orbital neoplasms in children and 3% to 9% of all orbital masses, making them the most common orbital tumor; some reports say they account for about 2% of all orbital tumors1). Osseous choristoma is a relatively rare subtype, accounting for about 0.1% of all conjunctival tumors and 1.7% to 5% of all ocular choristomas2).
Choristomas are further subclassified into dermoid, dermolipoma, single-tissue choristoma, and complex choristoma4).
QHow are a dermoid cyst and an epidermoid cyst different?
A
A dermoid cyst has a keratinizing stratified squamous epithelium lining the cyst wall and contains appendage structures such as hair follicles, sebaceous glands, and sweat glands. By contrast, an epidermoid cyst does not have appendage structures and the cavity is filled only with keratinized material (debris-like contents). When tissues derived from the endoderm, mesoderm, and ectoderm are all present together, it is called a teratoma.
Orbital dermoid cysts are broadly divided into three types according to the site of origin: superficial, deep, and dumbbell.
Type
Common site
Main symptoms
Superficial type (anterior type)
Lateral eyebrow and orbital rim
Painless subcutaneous mass
Deep type (deep intraorbital type)
Deep orbit, intraconal
Proptosis, displacement, and restricted eye movement
Dumbbell-shaped
Extending across the inside and outside of the orbital bone
With bone destruction
Common sites are the sutures of the zygomatic and frontal bones, and the frontozygomatic suture is the most common, accounting for about 60% of cases. The frontolacrimal suture accounts for about 25%.
Main findings: Proptosis, ocular deviation, and limited eye movement.
Inflammation: Lipogranulomatous inflammation may occur when the cyst leaks or ruptures.
Shape: A dumbbell-shaped lesion that extends across the orbital bone on both sides is accompanied by bone destruction. If it arises within the muscle cone, imaging is essential1).
The cause of orbital dermoid cysts is the trapping of embryonic ectoderm during fetal development.
Entrapment of embryonic epithelial buds: When fetal suture lines close during embryogenesis, epithelial buds derived from ectoderm become trapped in the bony suture line and form a cyst. This is the basic mechanism of choristoma.
Common suture sites: The frontozygomatic suture is the most common (about 60%). About 25% also occur at the frontolacrimal suture.
Dumbbell shape: It may take a shape spanning the inner and outer aspects of the orbital wall. Some grow while eroding bone.
Slow enlargement: It gradually enlarges with age, and symptoms may become apparent after adolescence.
Adult-detected cases: Although congenital, it may remain asymptomatic in childhood and be found in adulthood.
Among benign orbital tumors, dermoid cysts and epidermoid cysts are common and are among the representative diseases of pediatric orbital tumors.
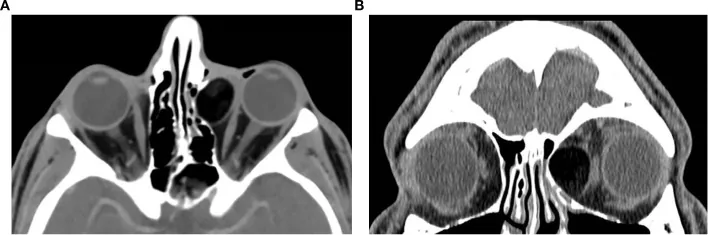
Levanon E, Greenberg G, Lustig-Barzelay Y, et al. Orbital masses: a review of CT imaging characteristics. Front Ophthalmol (Lausanne). 2025;5:1685141. Figure 5. PMID: 41323232; PMCID: PMC12660082; DOI: 10.3389/fopht.2025.1685141. License: CC BY.
Axial (a) and coronal (b) contrast-enhanced CT show a well-defined fat-attenuation lesion (about -105 HU) adjacent to the left medial rectus muscle, with thinning and outward bowing (bone scalloping) of the adjacent ethmoid inner plate. This corresponds to the CT findings discussed in section “4. Diagnosis and Examination Methods” (a clearly defined cystic mass, fat signal, and bone remodeling).
Superficial cysts can be diagnosed relatively easily from clinical findings such as their position along a suture line and their firm texture. Imaging is essential for deep cysts.
Well-defined cystic mass. Bone remodeling is seen in 85%.
MRI
Heterogeneous T1 and T2 signals (reflecting mixed fat and fluid). Low signal on fat-suppressed T1
Ultrasound
Mixture of low-reflective areas and irregular spike reflections
CT: Appears as a well-defined, capsulated cystic mass with homogeneous contents. Bone destruction or a bone defect may be seen1). It is useful for detecting a dumbbell shape and is also used to assess intracranial extension.
MRI: Because the cyst contents mix water-like and fat-like properties, signal intensity is heterogeneous on both T1-weighted and T2-weighted images1). It shows low signal on fat-suppressed T1 and is useful for confirming the fat component. It is excellent for detailed depiction of soft tissues and evaluation of surrounding neuromuscular structures.
Ultrasound: On A-scan, it shows a pattern with a mixture of low-reflective areas and irregular spike reflections.
Definitive diagnosis: Made by histopathological examination after excision. The inner surface of the cyst wall is lined by keratinized stratified squamous epithelium, and in dermoid cysts, adnexal structures such as hair follicles and sebaceous glands are identified.
Rhabdomyosarcoma: A rapidly growing malignant tumor. Differentiation is especially important.
Pleomorphic adenoma of the lacrimal gland: A solid mass in the superolateral orbit.
Paranasal sinus mucocele: A cystic lesion arising from the paranasal sinuses.
Congenital encephalocele and dacryocystocele: Differentiation from medial lesions.
QWhat does a dermoid cyst look like on CT or MRI?
A
On CT, it appears as a well-defined cystic mass, and bone remodeling is seen in 85% of cases. On MRI, it shows heterogeneous signal intensity on both T1 and T2, reflecting a mix of fat and fluid. It shows low signal on fat-suppressed T1, which is useful for identifying the fatty component.
Small, asymptomatic cysts may be managed with observation. However, they tend to enlarge with age, so regular follow-up and consideration of the right timing for surgery are necessary.
The principle is complete removal without rupturing the cyst wall. If any tissue remains, it can trigger sudden inflammation and cause recurrence, abscess formation, and an orbital cutaneous fistula.
Superficial excision
Incision site: choose from an eyebrow incision, an upper eyelid crease incision, or an incision directly over the lesion.
Key points of surgery: Complete excision without rupturing the cyst wall is essential. If the lesion is within the bone, removal with osteotomy is necessary. Because it is often strongly fused to the orbital bone, careful dissection is required.
Postoperative course: If complete excision is achieved, the prognosis is good and recurrence is rare.
Deep and complex excision
Orbital incision: choose a lateral approach or a combined anterior-lateral orbitotomy.
Intraconal: a transnasal endoscopic approach is also effective, and there is a report of complete removal of a 3.0 cm intraconal cyst1).
Dumbbell type: when it extends across the inside and outside of the orbital bone, coordination with neurosurgery is required. Perioperative planning that includes the intracranial component is important.
Limbal dermoid surgery: the main goal is cosmetic, and tumor excision and, if needed, superficial corneal transplantation (frozen-preserved cornea can be used; a trephine diameter of about 7.0 mm is often used) are performed.
QWhat happens if the cyst ruptures during surgery?
A
Lipids and keratin inside the cyst can leak out and cause lipogranulomatous inflammation. Copious irrigation during surgery can reduce the inflammation. Because incomplete removal can lead to recurrence, abscess formation, and an orbital cutaneous fistula, it is important to remove as much remaining tissue as possible even after rupture. Steroids are given after surgery to control inflammation.
QDoes a dermoid cyst keep growing?
A
It is a congenital lesion that slowly enlarges with age. Superficial lesions may remain asymptomatic for a long time, but if left untreated, the risk of eyelid compression, bone destruction, and cyst rupture increases. Deep lesions may cause symptoms such as proptosis and diplopia as they enlarge. It is important to discuss the timing of surgery with a specialist.
6. Pathophysiology and detailed mechanism of development
Orbital dermoid cysts are choristomas that arise when ectoderm is trapped at embryonic fusion lines. Skin-derived structures such as hair follicles, sebaceous glands, sweat glands, and keratinous material form ectopically within the orbit, where they do not normally belong.
Cyst formation: During embryonic fusion of the suture lines, epithelial buds derived from ectoderm become trapped within the bony sutures. The trapped epithelium continues to keratinize toward the lumen, forming adnexal structures such as hair follicles and sebaceous glands while the cyst grows.
Gradual enlargement: It slowly enlarges as keratinous material, hair, and sebum accumulate inside the cyst. It may cause pressure-related bone defects in the surrounding bone.
Inflammatory reaction: Leakage of keratin and lipids from the cyst wall triggers a severe inflammatory reaction in the surrounding tissue1). It presents as acute lipid granulomatous inflammation.
Pathological findings: The inner surface of the cyst wall is lined by keratinizing stratified squamous epithelium without atypia. In dermoid cysts, adnexal structures such as hair follicles and sebaceous glands are seen in the cyst wall.
Osseous choristoma: an unusual variant in which mature bone tissue is present within a dermolipoma4); proposed etiologic hypotheses include abnormal activation of pluripotent mesenchymal cells, reversion to a scleral bone plate, and developmental anomalies of the zygomaticofrontal suture2).
The intraconal epithelial cyst is an extremely rare subtype, accounting for only 0.5–0.6% of all orbital dermoid cysts, and only six cases were reported on PubMed from 1986 to 20201).
Samal et al. (2021) reported a 3.0 cm right intraconal dermoid cyst in a 30-year-old man1). Complete removal was achieved with a transnasal endoscopic approach, and there was no recurrence at 6 months. Pathology confirmed keratinizing stratified squamous epithelium and adnexal structures.
Minimally invasive surgical techniques, including the transnasal endoscopic approach, have been accumulating at the case-report level, and standardization is expected in the future.
Research on the histological diversity of choristomas is also advancing. Reported patterns include mixed bone-and-cartilage types, types containing tooth-like structures, and cartilaginous types with pigmented cystic change2). For osseous choristoma, proposed etiologic hypotheses include abnormal activation of pluripotent mesenchymal cells, reversion to a scleral bone plate, and developmental anomalies of the zygomaticofrontal suture2). For lacrimal gland choristoma, rare cases have been reported that include ectopic tissues such as cartilage, muscle, and nerve tissue within the lacrimal gland3), and the diverse tissue origins of choristomas are becoming clearer.
Samal S, Sable MN, Pradhan S, Pradhan P. Intraconal orbital dermoid cyst: a rare location. Autopsy & case reports. 2021;11:e2021282. doi:10.4322/acr.2021.282. PMID:34249789; PMCID:PMC8232379.
Zhong S, Fu J, Hu M, Zhang X, Cheng P. Epibulbar osseous choristoma. BMC ophthalmology. 2025;25(1):199. doi:10.1186/s12886-025-04024-9. PMID:40217468; PMCID:PMC11987218.
Cruz AAV, Limongi RM, Feijó ED, Enz TJ. Lacrimal gland choristomas. Arquivos brasileiros de oftalmologia. 2021;85(2):190-199. doi:10.5935/0004-2749.20220029. PMID:35416898; PMCID:PMC11826571.
Kim JM, Son WY, Sul HJ, Shin J, Cho WK. Epibulbar osseous choristoma with dermolipoma: A case report and review of literature. Medicine. 2022;101(47):e31555. doi:10.1097/MD.0000000000031555. PMID:36451416; PMCID:PMC9705003.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.