Obstructive sleep apnea (OSA) is a common sleep disorder in which the upper airway repeatedly becomes partially or completely blocked during sleep. This obstruction causes repeated cycles of hypoxemia and reoxygenation, leading to various systemic effects.
Apnea-hypopnea index (AHI) refers to the number of apnea and hypopnea events per hour of sleep. OSA is defined as AHI >5 accompanied by daytime sleepiness, fatigue, or cognitive impairment. Apnea is a complete cessation of airflow for at least 10 seconds, while hypopnea is a relative reduction in airflow accompanied by hypoxemia or arousal.
The prevalence is reported as 3–7% in men and 2–5% in women, but a US cohort reported 17–31% in men and 6.5–9% in women. Prevalence increases 2–3 times in those aged 65 and older. In children, it is more common with tonsillar and adenoid hypertrophy, and there is a higher tendency in African Americans.
OSA is recognized as an independent risk factor for ophthalmic diseases, and associations with six conditions—floppy eyelid syndrome, glaucoma, non-arteritic anterior ischemic optic neuropathy, papilledema, keratoconus, and central serous chorioretinopathy—have been reported (Huon 2016 [PMID 27230013], Bulloch 2024 [PMID 37227479]). Ophthalmologists involved in the care of OSA patients should keep these complications in mind.
QWhat eye diseases are more likely to occur with sleep apnea syndrome?
A
The main ophthalmic complications associated with OSA are six conditions: floppy eyelid syndrome, glaucoma, non-arteritic anterior ischemic optic neuropathy (NAION), papilledema, keratoconus, and central serous chorioretinopathy. Intermittent hypoxia, sympathetic overstimulation, and oxidative stress are involved as common pathophysiological mechanisms.
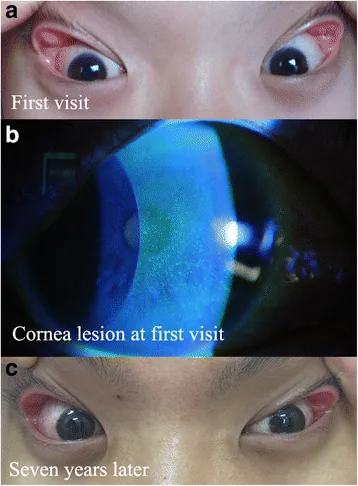
Superficial punctate keratopathy in a pediatric patient was related to adenoid hypertrophy and obstructive sleep apnea syndrome: a case report. BMC Ophthalmol. 2018 Feb 23; 18:55. Figure 1. PMCID: PMC5824558. License: CC BY.
Grade-2 floppy eyelids and mild bulbar conjunctival hyperaemia were noted in both eyes at the first visit (a). Scattered, fine, punctate corneal epithelial damage was confirmed by fluorescein staining of the right eye (b). The degree of floppy eyelid remained the same 7 years later (c)
Symptoms of OSA often begin insidiously, and several years may pass before a patient seeks medical attention. They worsen with weight gain, aging, and menopause.
Daytime symptoms:
Hypersomnia: Sleepiness that interferes with daily activities
Morning headache: Headache that occurs in the morning
Dry mouth and hypersensitivity: Symptoms associated with sleep fragmentation
Forgetfulness and depression: Effects on cognitive function and mood
Nighttime symptoms:
Snoring: Vibrational sound due to upper airway narrowing
Choking, gasping, or snorting sounds: Arousal response to airway obstruction
Ophthalmic complications associated with OSA are listed below.
FES
Floppy eyelid syndrome (FES): a condition in which the upper eyelid easily everts. OSA is present in a high proportion (90–100%) of patients with FES (Cristescu 2019 [PMID 31198891], Cheong 2023 [PMID 36427560]). The prevalence of FES in OSA patients is 4.5–18% (odds ratio 4.1).
Ocular surface symptoms: accompanied by papillary conjunctivitis, eyelid edema, and corneal epithelial erosion. Punctate epithelial keratitis is the most common.
Laterality: the affected eye tends to correspond to the side the patient sleeps on.
Association strength: OSA patients have a 16% higher incidence of non-arteritic anterior ischemic optic neuropathy. 71–89% of patients with non-arteritic anterior ischemic optic neuropathy have comorbid OSA. OSA increases the risk of non-arteritic anterior ischemic optic neuropathy by 1.7–3.8 times (Farahvash 2020 [PMID 32753994]).
Contralateral eye risk: In cases with comorbid OSA, the risk of developing non-arteritic anterior ischemic optic neuropathy in the contralateral eye also increases.
Glaucoma and Papilledema
Glaucoma: Prevalence in OSA patients is 2–27%. Nocturnal intraocular pressure elevation and oxidative stress after hypoxia are involved.
Papilledema: Bilateral optic disc swelling due to elevated intracranial pressure (ICP). In patients without risk factors for idiopathic intracranial hypertension (IIH), OSA should be considered in the differential diagnosis (Thurtell 2013 [PMID 23412355]).
Cornea and Retina
Keratoconus: Patients with keratoconus have a higher prevalence of OSA than the general population, and a meta-analysis has shown a significant association (Pellegrini 2020 [PMID 31895272]). It is more common in men with high BMI or a family history of OSA. Mechanical damage to the cornea during sleep has been proposed as a contributing factor.
Central serous chorioretinopathy (CSCR): About two-thirds of CSCR patients have comorbid OSA. Oxidative stress-induced vascular endothelial damage and vasoconstriction are involved.
QWhy can floppy eyelid syndrome cause symptoms in only one eye?
A
The affected eye tends to correspond to the side the patient usually sleeps on. It is thought that mechanical stimulation from the eyelid being pressed against the pillow or bedding in the lateral decubitus position leads to predominant ocular surface symptoms on that side.
OSA is also associated with the following systemic diseases: hypertension, metabolic syndrome, diabetes, heart failure, coronary artery disease, arrhythmias, stroke, pulmonary hypertension, neurocognitive disorders, and mood disorders.
Diagnosis is made using A to C below. It is confirmed when A or B and C are met. A definitive diagnosis is also made when AHI ≥15/hour regardless of symptoms.
A: Excessive daytime sleepiness that cannot be explained by other factors
B: Two or more of the following: choking or gasping during sleep, repeated awakenings, lack of restorative sleep, daytime fatigue, or difficulty concentrating
C: Five or more obstructive respiratory events per hour of sleep
Actively screen for FES during comprehensive ophthalmic examination in OSA patients
Clinical assessment of easy eyelid eversion is key to FES diagnosis
In the interview of patients with non-arteritic anterior ischemic optic neuropathy, confirm vascular risk factors, surgical history, smoking, medication history (such as PDE5 inhibitors), OSA symptoms, and giant cell arteritis symptoms.
QWhat tests are needed to diagnose sleep apnea syndrome?
A
The gold standard for definitive diagnosis is overnight polysomnography (PSG). For outpatient screening, the STOP-Bang questionnaire, Epworth Sleepiness Scale, and Berlin questionnaire are used. In FES patients, PSG is recommended when the ESS score is >10.
OSA treatment leads to fundamental management of ophthalmic complications.
Weight loss: The most basic management. Weight reduction improves AHI.
CPAP (continuous positive airway pressure) therapy: Prevents airway collapse during sleep. First-line treatment for OSA, effective in reducing symptoms and complications.
Oral appliance (mouthpiece): For mild OSA or patients intolerant to CPAP. Expands the airway by advancing the mandible or holding the tongue.
Surgery: Indicated for craniofacial abnormalities or clear obstructive lesions.
Hypoglossal nerve stimulation (HSN): For patients who do not respond to medical treatment. Reported to reduce AHI and ESS scores and improve arousal levels.
Side-sleeping: Conservative treatment by changing body position.
Ophthalmic care: Artificial tears and eye ointment instillation
Eyelid taping/eye shield: Prevents eyelid eversion during sleep
Avoid lateral and prone positions: Instruct patient not to sleep on the affected side
Anti-inflammatory eye drops: Use only short-term if ocular surface inflammation is severe
CPAP therapy: McNab reported that CPAP initiation led to resolution of papillary conjunctivitis and normalization of eyelid laxity. In moderate to severe OSA patients, 18 months of CPAP use showed statistically significant improvements in FES grade, OSDI score (dry eye symptoms), tear function tests (TBUT, Schirmer I), and corneal fluorescein staining.
Indicated for cases refractory to conservative therapy and CPAP.
Lateral tarsal strip (LTS): Reported 91% symptom improvement and 97.5% long-term stability in 70 cases.
Full-thickness wedge excision (FTWE): FTWE tends to have a higher recurrence rate compared to LTS.
A long-term study at Moorfields Eye Hospital (71 cases) reported recurrence rates of 25.6–60.6%, with medial and lateral canthoplasty and LTS showing better survival outcomes than FTWE.
Preventive Management for Nonarteritic Anterior Ischemic Optic Neuropathy
Identify and manage modifiable risk factors (hypertension, diabetes, hyperlipidemia, OSAS)
Recommend smoking cessation, weight loss, and exercise
Avoid taking nighttime antihypertensive medications before bedtime (nocturnal hypotension is a predisposing factor for nonarteritic anterior ischemic optic neuropathy)
Instruct the patient to avoid lying on the affected side
Consider intraocular pressure-lowering treatment if intraocular pressure is borderline or elevated
Check history of PDE5 inhibitor use (associated with risk of nonarteritic anterior ischemic optic neuropathy)
Perform intravitreal injections cautiously (rapid intraocular pressure elevation may impair ONH circulation and increase risk of contralateral nonarteritic anterior ischemic optic neuropathy)
QDoes CPAP therapy also improve eye symptoms?
A
CPAP has been shown to be effective for FES, with improvements in FES grade, dry eye symptoms, and tear function tests reported with long-term use (18 months or more). However, dry eye symptoms may temporarily worsen in the early stages of treatment, and continuation for more than one year is recommended. Its risk-reducing effect on non-arteritic anterior ischemic optic neuropathy has not been established at this time.
There are multiple hypotheses regarding the mechanism of FES onset.
Mechanical theory: During sleep in the lateral decubitus position, the eyelid inverts and the ocular surface comes into direct contact with the pillow or bedding. The fact that symptoms are strongest upon waking supports this theory.
Local ischemia-reperfusion theory (Culbertson & Tseng): A mechanism has been proposed involving eyelid compression ischemia in the lateral or prone position plus systemic intermittent hypoxia due to OSA, followed by reperfusion upon position change or awakening, leading to oxidative stress and free radical damage, connective tissue degeneration, and eyelid laxity.
Hyperleptinemia and matrix metalloproteinases (MMPs): Hyperleptinemia, which correlates with OSA severity, regulates MMP-9 expression in a dose-dependent manner. Increased MMP-7 and MMP-9 are involved in degeneration of the tarsal extracellular matrix. Histologically, decreased elastin content and collagen degeneration in the tarsus are observed.
Pathophysiology of nonarteritic anterior ischemic optic neuropathy
Glaucoma: Both vascular factors (oxidative stress during reperfusion after hypoxia) and mechanical factors (nocturnal intraocular pressure elevation due to sympathetic hypertonia) are involved.
CSCR: Oxidative stress-induced vascular endothelial damage and vasoconstriction lead to choroidal circulatory disturbance. Obesity may be a common risk factor.
7. Latest Research and Future Perspectives (Reports at Research Stage)
Research is progressing on this new option for patients who do not respond to medical treatment.
Current reports show that HSN therapy reduces AHI and ESS scores, improves arousal levels, and shortens wake after sleep onset. It is being considered for moderate to severe OSA patients intolerant to CPAP.
Bayir et al. reported that in patients with mild to moderate OSA who underwent anterior palatoplasty, the prevalence and grade of FES significantly decreased at 3 months postoperatively, and the oxygen desaturation index also improved. This finding suggests that surgical treatment of OSA itself may improve FES.
CPAP and Risk of Nonarteritic Anterior Ischemic Optic Neuropathy
Whether CPAP treatment reduces the risk of first-onset or contralateral eye onset of nonarteritic anterior ischemic optic neuropathy is currently not established. Further evidence accumulation is needed regarding the relationship between OSA management and prevention of nonarteritic anterior ischemic optic neuropathy.
Sergott et al. (1989) reported that optic nerve sheath decompression, which creates a slit or window in the tissue surrounding the optic nerve to drain CSF and resolve compartment syndrome, may offer the potential for visual improvement in cases of “progressive” nonarteritic anterior ischemic optic neuropathy. However, this procedure is not established as standard treatment and remains an investigational finding.
Farahvash A, Micieli JA. Neuro-Ophthalmological Manifestations of Obstructive Sleep Apnea: Current Perspectives.Eye Brain. 2020;12:61-71. doi:10.2147/EB.S247121. PMID: 32753994; PMCID: PMC7353992.
Bulloch G, Seth I, Zhu Z, Sukumar S, McNab A. Ocular manifestations of obstructive sleep apnea: a systematic review and meta-analysis.Graefes Arch Clin Exp Ophthalmol. 2024;262(1):19-32. doi:10.1007/s00417-023-06103-3. PMID: 37227479; PMCID: PMC10806133.
Huon LK, Liu SY, Camacho M, Guilleminault C. The association between ophthalmologic diseases and obstructive sleep apnea: a systematic review and meta-analysis.Sleep Breath. 2016;20(4):1145-1154. doi:10.1007/s11325-016-1358-4. PMID: 27230013.
Cheong AJY, Ho OTW, Wang SKX, et al. Association between obstructive sleep apnea and floppy eyelid syndrome: A systematic review and metaanalysis.Surv Ophthalmol. 2023;68(2):257-264. doi:10.1016/j.survophthal.2022.11.006. PMID:36427560.
Cristescu Teodor R, Mihaltan FD. Eyelid laxity and sleep apnea syndrome: a review.Rom J Ophthalmol. 2019;63(1):2-9. PMID: 31198891; PMCID: PMC6531778.
Pellegrini M, Bernabei F, Friehmann A, Giannaccare G. Obstructive Sleep Apnea and Keratoconus: A Systematic Review and Meta-analysis.Optom Vis Sci. 2020;97(1):9-14. doi:10.1097/OPX.0000000000001467. PMID: 31895272.
Thurtell MJ, Trotti LM, Bixler EO, et al. Obstructive sleep apnea in idiopathic intracranial hypertension: comparison with matched population data.J Neurol. 2013;260(7):1748-1751. doi:10.1007/s00415-013-6858-6. PMID: 23412355; PMCID: PMC3707935.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.