Refractive surgery (LASIK, PRK, RK, SMILE, etc.) alters corneal thickness and biomechanical properties. This change causes applanation tonometry to yield lower readings than actual intraocular pressure1).
Glaucoma can become a problem during long-term follow-up after refractive surgery. Postoperative underestimation of intraocular pressure can delay glaucoma diagnosis or overestimate treatment efficacy, making appropriate selection of pressure measurement methods clinically important2).
In patients with a history of refractive surgery, steroid-induced intraocular pressure elevation should also be considered. Even if intraocular pressure rises due to topical steroid use after LASIK, the measured value may remain within the normal range due to corneal thinning, risking oversight2).
Procedure
Effect on cornea
Effect on IOP measurement
LASIK
Stromal ablation + flap
Underestimation (large)
PRK
Surface ablation
Underestimation (moderate to large)
RK
Radial keratotomy
Underestimation (high variability)
QWhy is intraocular pressure measured lower after refractive surgery?
A
In refractive surgery, corneal stroma is removed to correct myopia, reducing central corneal thickness (CCT). The Goldmann applanation tonometer is designed based on a CCT of 520 μm; when the cornea is thinner, less force is required for applanation, leading to underestimation of intraocular pressure1). Additionally, in LASIK, flap creation reduces corneal structural strength and alters biomechanical properties, causing measurement errors that cannot be explained solely by changes in CCT.
3. Causes and Risk Factors for Intraocular Pressure Underestimation
The main cause of intraocular pressure measurement error after refractive surgery is thinning due to corneal stromal ablation. It is estimated that for every 10 μm of corneal ablation, intraocular pressure is underestimated by approximately 0.3–0.4 mmHg. In high myopia correction, the amount of ablation is larger, leading to greater underestimation.
In addition to changes in central corneal thickness, corneal viscoelastic properties (corneal hysteresis: CH) also change postoperatively. In LASIK, both flap creation and excimer laser irradiation affect corneal biomechanics1). A decrease in CH is an additional source of error in applanation tonometry.
After radial keratotomy (RK), incisional scars in the peripheral cornea cause flattening of the central cornea. In addition to changes in corneal curvature, there is a characteristic increase in diurnal variation. The cornea after RK is also sensitive to temperature changes; it bulges in the morning and flattens during the day, causing large fluctuations in intraocular pressure measurements.
Topical steroids prescribed after LASIK can increase intraocular pressure2). When underestimation due to corneal thinning and actual pressure elevation offset each other, measured values may remain within the normal range, and the pressure increase may go unnoticed 2). The use of a suction ring can also cause transient intraocular pressure elevation 2).
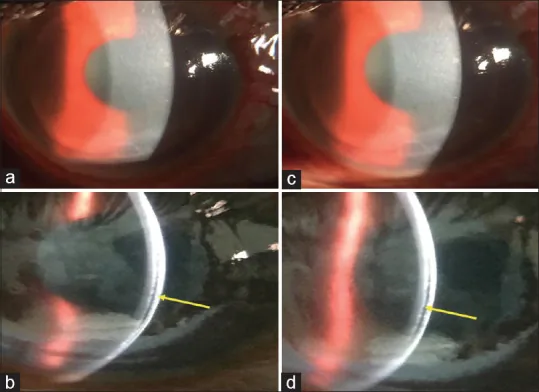
McHarg M, Denny M, Radhakrishnan S. Open-Angle Glaucoma Presenting as Delayed-Onset Interface Fluid Syndrome in a Patient With Minimal Risk Factors. Cureus. 2026;18:e103169. Figure 1. PMID: 41809309; PMCID: PMC12970951. DOI: 10.7759/cureus.103169. License: CC BY 4.0.
Anterior segment photograph and cross-sectional image showing interface fluid accumulation after LASIK. The difficulty of intraocular pressure assessment after refractive surgery is demonstrated.
Goldmann applanation tonometer (GAT): The clinical gold standard, but it is affected by corneal thickness and biomechanical properties 1). After refractive surgery, it underestimates intraocular pressure, so careful interpretation of measurements is necessary 1)2).
Non-contact tonometer (NCT): Uses an air puff to flatten the cornea; similar to GAT, it underestimates pressure postoperatively. Because it deforms the cornea rapidly, the influence of corneal biomechanics is greater than with GAT1).
Tonometer less affected by central corneal thickness
Principle: Measures intraocular pressure directly with a sensor tip that matches the corneal curvature contour
Postoperative accuracy: Allows measurements with minimal influence from central corneal thickness and corneal curvature, and is recommended for intraocular pressure measurement after refractive surgery 1)
Limitations: Tends to show higher values than GAT. Requires some skill to perform the measurement.
ORA (IOPcc)
Principle: Calculates intraocular pressure (IOPcc) corrected for corneal properties using corneal hysteresis.
Postoperative accuracy: IOPcc is reported to provide more accurate IOP estimation than GAT after refractive surgery 1).
Limitations: Tends to overestimate compared to GAT in high IOP ranges. Waveform quality verification is important.
Tonopen: A portable tonometer that measures with a tip pressure transducer. Some reports indicate it is more reliable than GAT for IOP measurement after LASIK. However, there is a risk of missing elevated IOP, so its use alone is not recommended.
iCare rebound tonometer: Can measure without topical anesthesia. It is affected by central corneal thickness, but some reports suggest the effect is smaller than with GAT.
QWhich tonometer is most suitable for measuring intraocular pressure after refractive surgery?
A
Dynamic contour tonometry (DCT) is least affected by corneal properties and is recommended for measuring intraocular pressure after refractive surgery 1). The ORA IOPcc, which uses corneal hysteresis for correction, is also useful for estimating postoperative intraocular pressure1). However, it is advisable not to rely solely on a single tonometer but to combine multiple measurement methods for a comprehensive evaluation when possible. Comparison with preoperative central corneal thickness and IOP records is also important 2).
6. Pathophysiology of Intraocular Pressure Underestimation
GAT calculates intraocular pressure from the force required to flatten the cornea over a diameter of 3.06 mm, based on the Imbert-Fick law 1). This law assumes the cornea is an ideal thin membrane, but the actual cornea has thickness, rigidity, and viscoelasticity. When the cornea becomes thinner after refractive surgery, the force required for flattening decreases, leading to underestimation of intraocular pressure.
The corneal stroma is a viscoelastic body composed of collagen fibers and matrix (glycosaminoglycans and proteoglycans). Excimer laser ablation reduces the number of collagen lamellae and decreases corneal elasticity 1). LASIK flap creation further cuts Bowman’s membrane on the anterior cornea, compromising structural strength.
In corneal edema (pathologically thick cornea), increased tissue water content softens the cornea, leading to underestimation of intraocular pressure by GAT1). Conversely, physiologically thick corneas are overestimated by GAT. After refractive surgery, both thinning and biomechanical changes are involved, making it difficult to predict measurement error solely from changes in central corneal thickness.
A complication specific to LASIK is interface fluid syndrome (IFS). This condition involves fluid accumulation at the flap interface, often associated with steroid-induced intraocular pressure elevation or uveitis. Because the flap is elevated by fluid, GAT may show normal or low intraocular pressure, but there may actually be significant intraocular pressure elevation.
If IFS is suspected, observation of the flap interface using anterior segment OCT or slit lamp is important. Emergency intraocular pressure-lowering treatment may be required.
QWhat is interface fluid syndrome?
A
Interface fluid syndrome (IFS) is a condition in which fluid accumulates at the flap interface after LASIK. The main cause is steroid-induced intraocular pressure elevation, and because the flap is lifted by the fluid, Goldmann applanation tonometry (GAT) shows an apparently normal intraocular pressure. However, the actual intraocular pressure may be significantly elevated, posing a risk of optic neuropathy. Detection of interface fluid by anterior segment OCT and treatment to lower intraocular pressure, including discontinuation of steroids, are necessary.
Development of intraocular pressure measurement methods that consider corneal biomechanics is progressing. The Corvis ST uses a high-speed Scheimpflug camera to record corneal deformation induced by an air jet as a video and calculates numerous biomechanical parameters 1). It is expected to be applied to more accurate intraocular pressure estimation by analyzing corneal deformation patterns after refractive surgery.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL, et al. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153(5):789-803.e2. PMID: 22245458.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.