Brown-McLean syndrome is a disease in which edema occurs in the peripheral inferior cornea (2–3 mm from the limbus) and progresses circumferentially. The central cornea is spared in most cases.
It was first reported in 1969 by Brown and McLean as “peripheral corneal edema after cataract extraction.” It was later named as a distinct disease and remains so today.
It is a relatively rare disease, classically reported more frequently in aphakic eyes after intracapsular cataract extraction (ICCE). It is known to develop on average 6 to 16 years after surgery. Most patients are elderly, but cases as young as 12 years old have been reported.
High myopia has been reported in association with Brown-McLean syndrome, with a prevalence of 40–61%.
QHow long after cataract surgery does it develop?
A
It develops after a long latent period averaging 6 to 16 years postoperatively. Therefore, when examining elderly patients with a history of cataract surgery, it is important to check the peripheral cornea even if the surgery was performed long ago.
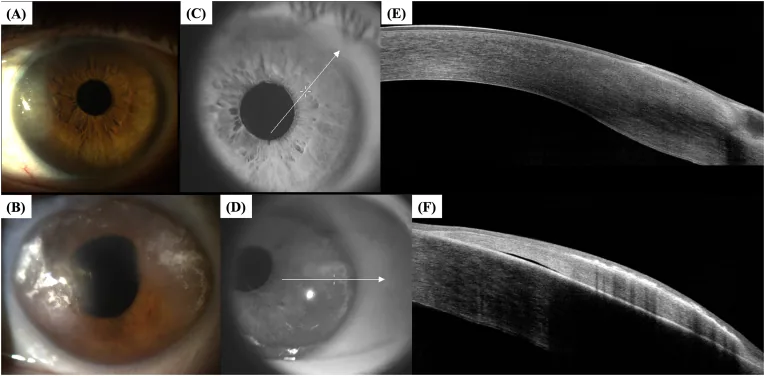
Guedes J, et al. Biomechanical and tomographic findings in Brown-McLean syndrome. Am J Ophthalmol Case Rep. 2024. Figure 6. PMCID: PMC11359765. License: CC BY.
Anterior segment slit-lamp photographs of the right eye (A) and left eye (B) of Case 3, and anterior segment optical coherence tomography (AS-OCT) images of the right eye (E) and left eye (F) taken along the scan lines in (C) and (D). These correspond to the peripheral corneal edema discussed in the section “2. Main Symptoms and Clinical Findings.”
Usually asymptomatic. When symptoms appear, the following are common.
Foreign body sensation: May be perceived as peripheral edema progresses.
Photophobia (sensitivity to light): Observed when inflammation or edema worsens.
Decreased visual acuity: Minimal impact on vision as long as the central cornea is preserved. In severe cases with central corneal decompensation, visual loss becomes significant.
Slit-lamp examination is central to diagnosis. Characteristic findings are shown below.
Peripheral Findings
Peripheral corneal edema: Initially begins in the inferior periphery including the limbus, progressing circumferentially. The superior cornea is generally spared, though rare cases present with edema starting superiorly.
Brown to orange endothelial pigmentation: Characteristic pigmentation is observed on the corneal endothelium in the edematous area. This is thought to be caused by intermittent endothelial trauma due to iridodonesis.
Iris atrophy: Atrophy of the iris directly beneath the area of corneal edema has been reported.
Central/Overall Findings
Maintenance of central corneal transparency: Guttae are rarely observed in the central cornea, and endothelial cell density is maintained within normal limits. 1)
Iridodonesis: Commonly observed in aphakic eyes, causing intermittent endothelial trauma.
Angle pigmentation: Gonioscopy reveals a wide, deep angle with varying degrees of pigmentation on the trabecular meshwork.
It has been reported that while the central corneal thickness remains normal (e.g., 541 μm), the edematous peripheral areas (nasal and temporal sides) show thickening exceeding 700 μm. 1)
Transient central corneal swelling associated with elevated intraocular pressure may be observed, but persistent central edema is rare and limited to severe cases.
When Brown-McLean syndrome occurs in a transplanted cornea, it has been confirmed that pigmentation and edema begin near the center of the donor cornea, with a clear peripheral zone present just before the graft-host junction.
QCan vision be significantly reduced in Brown-McLean syndrome?
A
Since the central cornea is preserved, the impact on vision is often minimal. However, if left untreated and progression leads to central corneal decompensation, corneal transplantation may become necessary. Additionally, rupture of associated epithelial bullae poses a risk of infectious corneal ulcers.
The pathophysiology of Brown-McLean syndrome remains unclear. Initially, an association with potential corneal endothelial dystrophy was suspected, but no specific dystrophy or gene has been identified. Cases within families suggest a possible genetic predisposition. 2)
Main risk factors and related procedures are as follows:
Aphakic eyes after intracapsular cataract extraction: the most classic and typical background for onset
Homocystinuria: onset of Brown-McLean syndrome has been reported in cases of lens subluxation or aphakia associated with this metabolic disease 2)
Iridodonesis: Thought to cause intermittent corneal endothelial trauma and promote onset.
It has also been shown that endothelial trauma is not necessarily required for the development of Brown-McLean syndrome; there are cases without iridocorneal contact on ultrasound biomicroscopy (UBM) and cases that developed even after iridectomy. 2)
Diagnosis is based on a combination of clinical findings from slit-lamp examination and medical history. Brown-McLean syndrome is suspected in patients with a history of intraocular surgery such as intracapsular cataract extraction, or a history of non-surgical conditions (e.g., lens subluxation), who present with corneal edema extending from the inferior periphery to the entire circumference.
Specular microscopy (corneal endothelial cell examination): Endothelial cell count and morphology in the central cornea remain normal. In the peripheral cornea, the endothelium often shows decreased cell count and morphological changes, but may also be normal. Panoramic imaging with wide-field specular microscopy has confirmed that high-density cells are uniformly distributed up to the boundary between edematous and non-edematous areas. 1)
In vivo confocal microscopy: In the peripheral cornea, corneal nerve hypertrophy, Bowman’s layer fibrosis, and irregular shape and size of basal epithelial cells may be observed. The central corneal endothelium is generally normal, and reports have noted large keratocytes and thick corneal nerves in the posterior stroma.
Anterior segment optical coherence tomography (AS-OCT): Allows quantitative assessment of peripheral corneal thickening. For example, a marked difference of over 700 μm in the periphery and 541 μm in the center has been recorded. 1)
Scheimpflug imaging: Allows simultaneous confirmation of peripheral corneal thickening and normal central thickness.
Electron microscopy: In the peripheral cornea of Brown-McLean syndrome, abnormal posterior collagen layer and disrupted endothelial cells are observed in Descemet’s membrane. Scanning electron microscopy may show a clear demarcation line between normal and pathological endothelium.
Gonioscopy: The angle is wide and deep, with varying degrees of pigmentation in the trabecular meshwork. In eyes with inferior corneal edema, it is also important to check for foreign bodies or retained lens material via gonioscopy.
QHow to differentiate Brown-McLean syndrome from Fuchs endothelial corneal dystrophy?
A
In Fuchs endothelial corneal dystrophy, guttae occur in the central cornea and edema starts centrally, whereas in Brown-McLean syndrome, guttae are rarely seen in the central cornea and edema begins from the inferior periphery. A history of intraocular surgery is also an important clue for diagnosing Brown-McLean syndrome.
Most cases of Brown-McLean syndrome respond to conservative treatment.
Hypertonic saline eye drops: Use 5% sodium chloride eye drops or ointment. Aimed at osmotic reduction of corneal edema. In one case, NaCl 5% ointment was used at bedtime, and corrected visual acuity improved from 20/160 to 20/80 after 6 months. 2)
Topical steroid eye drops: Used to reduce edema and suppress inflammation.
It has also been shown that contact lens wear may be well tolerated even in the presence of peripheral corneal edema.
Surgery is considered for refractory cases or when symptoms are pronounced.
Annular amniotic membrane transplant: For recurrent epithelial bullae secondary to Brown-McLean syndrome, annular amniotic membrane transplantation using two trephines of different diameters, with the basement membrane side of the amniotic membrane facing upward, is considered effective. It allows treatment of bullae while maintaining central vision.
Anterior stromal puncture: Performed using a 23G or 25G needle. It induces collagen expression, improves epithelial cell adhesion and subepithelial fibrosis, thereby enhancing the barrier function against water entry into the corneal epithelium.
In Brown-McLean syndrome, the central corneal endothelial cells (CEC) maintain high density, while the peripheral endothelium is damaged. In Fuchs endothelial corneal dystrophy, it was generally thought that a decrease and enlargement of endothelial cells begin in the central area and progress toward the periphery. 1) In contrast, Brown-McLean syndrome shows the opposite pattern: the peripheral endothelium is selectively damaged, while the high-density central endothelium remains stable over a long period.
In a 12-year long-term follow-up case, the central CEC density was 2,499 cells/mm² at the initial visit and 2,456 cells/mm² after 12 years, showing almost no change, with an annual decrease rate of only 0.09%. 1)
The following hypotheses have been proposed to explain this unique distribution. 1)
Formation of a biological barrier: A structure similar to Schwalbe’s line (corneal border line) may accidentally form in the periphery, preventing cell migration from the center to the periphery.
Selectivity in endothelial cell migration direction: Corneal endothelial cells may prefer centripetal (toward the center) migration and have limited ability for centrifugal (toward the periphery) migration.
Migration inhibition by degenerated cells: Degenerated endothelial cells in the edematous area may physically obstruct cell migration from the center to the periphery.
It has been hypothesized that trauma to the endothelium, in addition to a genetic predisposition to corneal endothelial disease, may cause Brown-McLean syndrome. Iridodonesis is thought to cause intermittent endothelial trauma, selectively damaging the peripheral endothelium.
Ultrasound biomicroscopy sometimes shows no iridocorneal contact, indicating that endothelial trauma is not necessarily required for the development of Brown-McLean syndrome.
When corneal endothelial damage progresses and the pump and barrier functions of the endothelium fall below a threshold, the water content of the corneal stroma increases, leading to edema. In Brown-McLean syndrome, this damage is characteristically limited to the periphery.
QWhy does the central cornea remain clear for a long time?
A
There is no clear answer at present. It has been proposed that a biological barrier (Schwalbe’s line-like structure) may form at the border between the central and peripheral regions, or that endothelial cells may have a property that makes it difficult for them to move centrifugally (from center to periphery). 1) Elucidating this mystery could lead to the development of new treatments for corneal endothelial diseases.
7. Latest Research and Future Prospects (Investigational Reports)
Long-term follow-up over 12 years suggests that a biological barrier may form at the boundary between the central and peripheral areas in Brown-McLean syndrome. 1) If this hypothesis is confirmed, treatment approaches that intentionally create similar mechanical barriers could be considered. This may provide new perspectives for understanding and developing treatments for corneal endothelial diseases in general.
Tomioka et al. (2024) reported a 12-year long-term follow-up case at Kyoto Prefectural University of Medicine. 1) Panoramic images using slit-scanning wide-field contact specular microscopy confirmed that high-density CEC was uniformly distributed up to just before the boundary between edematous and non-edematous areas, comparable to the central area. The extremely stable course with an annual central CEC decrease rate of 0.09% suggests unique endothelial cell dynamics in Brown-McLean syndrome.
Recognition of cases with systemic diseases such as homocystinuria
It has been reported that patients with metabolic diseases such as homocystinuria may develop Brown-McLean syndrome after lens subluxation or aphakia. 2) Establishing a diagnostic and follow-up protocol for such cases with systemic complications is considered a future challenge.
Alenezi et al. (2021) reported the first case of Brown-McLean syndrome associated with homocystinuria in the Middle East. 2) A 29-year-old male developed the condition in his left eye more than 22 years after vitrectomy and lensectomy for bilateral lens subluxation. Conservative treatment with 5% NaCl ointment improved corrected visual acuity from 20/160 to 20/80. Additionally, the presence of a large inferior iridectomy did not prevent the development of inferior peripheral edema, which is an important finding that refutes the conventional hypothesis of a protective role for superior iridectomy.
Tomioka Y, Tanaka H, Sotozono C, Kinoshita S. A comprehensive long-term follow-up study of Brown-McLean syndrome. American journal of ophthalmology case reports. 2024;36:102146. doi:10.1016/j.ajoc.2024.102146. PMID:39282598; PMCID:PMC11393604.
Alenezi SH, Alrefaie SM, Alreshidi SO, ALBalawi HB, Osorio HM.. Brown-Mclean syndrome in an aphakic patient with homocystinuria: The first reported case in Middle East. Saudi J Ophthalmol. 2020;34(4):300-302. doi:10.4103/1319-4534.322619. PMID:34527877; PMCID:PMC8409359.
Chatterjee S, Parchand SM, Dash D, Agrawal D. Brown-McLean syndrome revisited. Indian J Ophthalmol. 2020;68(1):183-184. PMID: 31856505.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.