Tubulointerstitial nephritis and uveitis syndrome (TINU) is a rare systemic inflammatory disease that combines acute tubulointerstitial nephritis (TIN) and bilateral uveitis. It was first reported by Dobrin et al. in 1975 1). In the early 21st century, only about 133 cases were reported worldwide, but since then the number of case reports has increased, reaching approximately 600 cases 1).
It is considered an immune-mediated disease involving a common autoantigen in the kidney and eye, and it predominantly affects adolescent females. Renal and ocular symptoms often appear at different times, leading to delayed diagnosis.
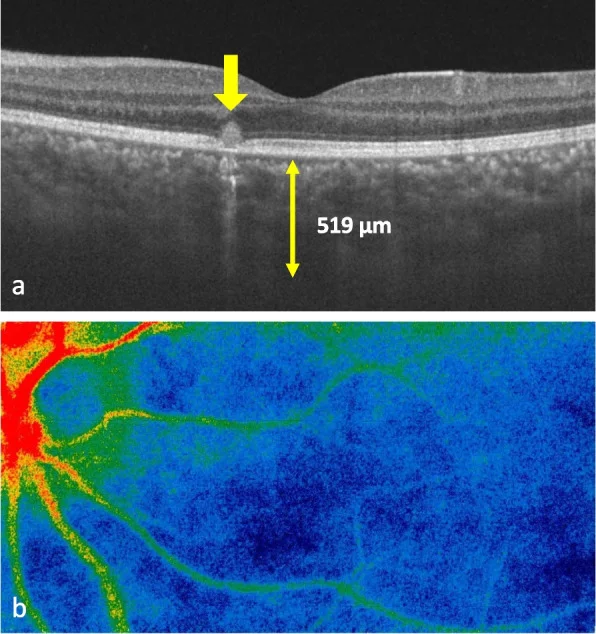
Arita T, et al. A case of tubulointerstitial nephritis and uveitis syndrome accompanied by subclinical choroiditis. BMC Ophthalmol. 2023. Figure 2. PMCID: PMC10588062. License: CC BY.
Swept-source OCT shows choroidal thickening to 519 μm and hyperreflective lesions adjacent to the retinal pigment epithelium level. The LSFG color map shows a cold-color-dominant pattern indicating decreased choroidal blood flow. This corresponds to the posterior segment inflammatory findings associated with TINU syndrome discussed in section “4. Clinical Features”.
The incidence is estimated at 1–2 cases per million per year 1). It accounts for 0.1–2% of uveitis patients, and about 5% of TIN biopsy cases show this syndrome 2). In children, it is one of the main causes of uveitis along with ocular sarcoidosis and juvenile chronic iridocyclitis.
Epidemiologically, it predominantly affects young women. A 2022 systematic review reported a median age of onset of 17 years and a female-to-male ratio of 1.8:1 1). However, recent reports indicate that with increased diagnostic awareness, cases are also being diagnosed in adults and the elderly 1)3). A study from Northern Ireland reported a mean diagnostic age of 43 years 3). No specific ethnic, racial, or geographic associations have been established.
QHow rare is TINU syndrome?
A
The annual incidence is estimated at 1–2 cases per million people. It accounts for only 0.1–2% of all uveitis cases, and it is believed that a considerable number of undiagnosed cases are actually labeled as idiopathic1).
The exact pathogenesis of TINU syndrome is not fully understood, but it is considered an autoimmune disease involving both humoral and cellular immunity1)4).
Histological findings from renal biopsies show that the predominant infiltrating cells are helper/inducer T cell subsets3). This suggests that cellular immunity plays a central role in the pathogenesis.
Humoral immunity involvement has also been reported. Tan et al. detected serum anti-modified CRP (mCRP) antibodies at a high rate in 9 patients with TINU syndrome, suggesting that mCRP may be a common target autoantigen in renal and ocular tissues4).
Renal tubular epithelium and ocular ciliary epithelium have embryologically similar structures. Dysfunction of enzymes common to both tissues or targeted destruction by immune responses is hypothesized as the mechanism for simultaneous kidney and eye involvement.
A strong association with specific HLA genotypes has been reported. Levinson et al. identified the HLA-DQA101/DQB105/DRB1*01 haplotype in 13 of 18 patients1). In Japanese patients, associations with HLA-A2, HLA-A24, HLA-A31, and HLA-DR4 have been noted4). It is speculated that these HLA class II molecules are involved in presenting autoantigens and activating autoreactive T cells.
Drug-induced tubulointerstitial nephritis can trigger the onset of TINU. In a review by Mandeville et al., approximately 24% of reported cases had a history of antibiotic use, and 18% had a history of NSAID use4). The following drugs have been reported as causative agents:
Antibiotics: rifampicin, sulfonamides, etc.
NSAIDs: ibuprofen, etoricoxib, etc.
Antiepileptic drugs
Peptic ulcer drugs
Prior infections with Epstein-Barr virus, varicella-zoster virus, and Chlamydia have been suggested as triggers 1). Cases associated with SARS-CoV-2 infection have also been reported, with viral spike protein detected in kidney tissue 5). Co-occurrence with autoimmune diseases such as hyperthyroidism and rheumatoid arthritis has been described 1)4).
Cunha et al. (2026) reported a case series of four patients; one had a history of rheumatoid arthritis and NSAID use, and another had preceding viral gastroenteritis. This report highlighted the diversity of environmental factors 1).
TINU syndrome presents with systemic, renal, and ocular symptoms. The onset of these three components often occurs at different times, making diagnosis challenging.
Reflecting acute tubulointerstitial nephritis, it may be asymptomatic. It is often detected by laboratory abnormalities such as elevated serum creatinine, proteinuria, sterile pyuria, and glycosuria. Severe cases may lead to acute kidney injury requiring dialysis, but renal prognosis is generally good.
Photophobia (sensitivity to light): Occurs depending on the degree of inflammation.
Decreased vision: Occurs due to anterior chamber inflammation or complications.
Approximately 80% present as acute-onset bilateral non-granulomatous anterior uveitis1). Uveitis is accompanied by anterior chamber cells and flare, with 65% being bilateral and 88% being anterior uveitis1). In recurrent or persistent cases, mutton-fat KP, fibrin exudation, posterior synechiae, and hypopyon may be observed.
Typical findings
Anterior chamber cells and flare: Inflammatory findings in the anterior chamber. The degree is often mild to moderate.
Keratic precipitates (KP): Mostly fine punctate KP, but some cases present with mutton-fat KP.
Posterior synechiae: Occurs in chronic cases.
Posterior segment findings
Optic disc swelling: observed in approximately 33% of cases, suggesting progression to posterior uveitis6).
Vitreous opacities: vitreous cells are seen in about 22% of cases6).
Retinal exudates: appear in approximately 11% of cases6).
There is a time lag between the onset of ocular and renal symptoms. In 65% of cases, ocular symptoms appear after renal symptoms, in 21% they precede, and in 15% they occur simultaneously. Ocular symptoms may appear up to 14 months after renal diagnosis1), and this time lag is a major factor making diagnosis difficult.
QAre there ocular complications other than anterior uveitis?
A
Approximately 20% of cases present with intermediate, posterior, or panuveitis. Reports include optic disc swelling, vitreous opacities, choroidal neovascularization, and neuroretinitis6)7)2). Although rare, these can lead to severe visual impairment, so thorough examination of the posterior segment is recommended.
Important laboratory findings for evaluating nephritis are as follows.
Elevated urinary β2-microglobulin: A sensitive marker of tubular damage. It often shows abnormally high levels more than 10 times the reference value and is considered the most useful diagnostic marker. It may be elevated even when serum creatinine is within the normal range 3). However, it is elevated in TIN in general and is not specific to TINU syndrome 1).
Urinary β-N-acetylglucosaminidase (NAG) level: A reference marker for tubular damage.
Proteinuria: Tubular low-molecular-weight proteinuria, observed in 68% of cases 3).
Sterile pyuria: Observed in 42% of cases 3).
Glycosuria: Normoglycemic glycosuria occurs in 34–47% of cases 3).
A definitive diagnosis of TIN can only be made by kidney biopsy4). Typical histological findings are as follows:
Inflammatory cell infiltration in the renal interstitium, mainly lymphocytes, plasma cells, and macrophages
Eosinophil infiltration (34%) and neutrophil infiltration (25%) are also observed1)
Glomeruli and blood vessels are preserved
No immune deposits are detected by immunofluorescence1)
QIs kidney biopsy always necessary?
A
Kidney biopsy is necessary for a definitive diagnosis, but in mild kidney disease, the risks may outweigh the benefits. If there is high urinary β2-microglobulin and typical bilateral anterior uveitis, a diagnosis of “presumed case” can be made7). The decision is made in consultation with a nephrologist.
Treatment of TINU syndrome involves both ocular inflammation and renal inflammation. Collaboration between ophthalmology and nephrology is important. The uveitis treatment guidelines also recommend collaboration with nephrology for TINU syndrome as a differential diagnosis of pediatric uveitis8).
For anterior uveitis, the following topical treatments are performed.
Steroid eye drops: Dexamethasone or betamethasone eye drops are used. The frequency is adjusted according to the degree of inflammation and gradually tapered 4).
Mydriatics (pupil management): Tropicamide/phenylephrine (Mydrin P) or cyclopentolate is used. The aim is to prevent posterior synechiae and reduce pain.
If renal function does not normalize promptly, systemic administration of corticosteroids is performed.
Oral prednisolone: Started at 1 mg/kg/day and tapered according to clinical response 1).
Intravenous methylprednisolone pulse: In severe cases, 500 mg to 1 g/day is administered for 3 to 5 days, followed by oral administration in some cases 1).
If there are drugs that may be triggers, such as rifampicin or sulfonamides, they should be discontinued.
Second-line therapy (steroid-resistant or side-effect cases)
For uveitis, the use of TNFα inhibitors (adalimumab) has also been reported in cases unresponsive to steroid eye drops or when steroid tapering is difficult 1)7). When uveitis becomes severe with retinal vasculitis or recurs, oral steroids or immunosuppressive agents are required.
Nephritis generally follows a favorable course. Steroid treatment for nephritis can be discontinued after a median of about 8 months 7). In most cases, renal function recovers completely, but progression to chronic kidney disease has been reported in some cases.
Treatment for uveitis requires a longer duration (median 18 months) than for nephritis 7). Up to 40% of cases experience recurrence and tend to become chronic. Recurrence can lead to complications such as flare-up of anterior chamber inflammation, posterior synechiae, secondary glaucoma, and cataracts. Long-term follow-up in anticipation of recurrence is recommended.
Steroid treatment for nephritis can be discontinued after a median of about 8 months. On the other hand, treatment for uveitis requires a longer period, with a median of 18 months7). Long-term follow-up is recommended in case of recurrence.
Latest Research and Future Perspectives (Investigational Reports)
García-Fernández et al. (2023) detected SARS-CoV-2 spike protein by immunofluorescence in renal biopsy tissue from a 12-year-old girl with TINU5). Viral protein was persistently detected in two renal biopsies performed at 3 and 10 months after symptom onset. It was suggested that renal tropism of SARS-CoV-2 may be involved in the onset and exacerbation of TINU.
Detection of Occult Choroiditis by Multimodal Imaging
Arita et al. (2023) detected occult choroiditis, which is difficult to detect by routine fundus examination, using multimodal imaging (ICG angiography, OCT, laser speckle flowgraphy) in a 12-year-old boy with TINU 6). This suggests that latent posterior segment inflammation may exist in TINU syndrome, and detailed imaging is recommended from the perspective of preventing choroidal neovascularization (CNV).
Vazquez et al. (2024) reported a 12-year-old girl who developed neuroretinitis 21 months after TINU diagnosis despite treatment with methotrexate and adalimumab7). Visual acuity recovered to 20/20 after switching to high-dose steroids and infliximab. This case demonstrates that new ocular complications can occur even under immunosuppression.
Monocyte chemoattractant protein-1 (MCP-1) is elevated in the urine of TIN patients and has been reported to correlate with disease activity 4). Its application in monitoring and severity assessment of TINU syndrome is expected in the future.
TINU and Monoclonal Gammopathy in Elderly Patients
Zhang et al. (2025) reported a case of TINU syndrome complicated with monoclonal gammopathy of undetermined significance (MGUS) in a 74-year-old woman 3). Renal biopsy confirmed acute interstitial nephritis, with κ light chain deposition in the vessel walls, but no MIg deposition in glomeruli or tubules. Glucocorticoid treatment improved the renal impairment due to TINU.
Cunha J, Afonso R, Calças Marques R, Cabrita A, Paula Silva A.. Clinical Presentation and Management of Tubulointerstitial Nephritis and Uveitis Syndrome: A Case Series. Cureus. 2026;18(1):e101107. doi:10.7759/cureus.101107. PMID:41658682; PMCID:PMC12882806.
Paroli MP, Cappiello D, Staccini D, Tamburrelli AC, Paroli M, Iannetti L.. Juxtapapillary Choroidal Neovascularization in a Young Woman with Tubulointerstitial Nephritis and Uveitis (TINU) Syndrome with Onset in Pediatric Age. Medicina (Kaunas). 2022;58(9):1260. doi:10.3390/medicina58091260. PMID:36143936; PMCID:PMC9503526.
Zhang JH, Liu J, Chen Q, Ruan DD, Liao LS, Lin KP, Zheng XL, Luo JW, Zhang L.. A rare concurrence of monoclonal gammopathies in an older adult with tubulointerstitial nephritis and uveitis syndrome. BMC Geriatr. 2025;25(1):472. doi:10.1186/s12877-025-06151-w. PMID:40604560; PMCID:PMC12219943.
Farnan R, Leavey S, Stokes J, Casey R.. Tubulointerstitial nephritis and uveitis syndrome: an unexpected diagnosis. BMJ Case Rep. 2025;18(12):e263098. doi:10.1136/bcr-2024-263098. PMID:41386977; PMCID:PMC12712788.
Sonia García-Fernández, Eva Fernández-Morán, Cecilia López-Martínez, Blanca Vivanco-Allende, Carmen Costales-Álvarez, Flor A. Ordóñez-Álvarez. Tubulointerstitial nephritis and uveitis syndrome and SARS-CoV-2 infection in an adolescent: just a coincidence in time?. Pediatr Nephrol. 2023;38(12):4203-4207. doi:10.1007/s00467-023-05950-w.
Arita T, Namba K, Iwata D, Suzuki K, Ogino Y, Mizuuchi K, Hiraoka M, Kitaichi N, Ishida S.. A case of tubulointerstitial nephritis and uveitis syndrome accompanied by subclinical choroiditis. BMC Ophthalmol. 2023;23(1):424. doi:10.1186/s12886-023-03172-0. PMID:37864178; PMCID:PMC10588062.
Vazquez SE, Niemeyer K, Mentreddy A, Gonzales J, Rasool N, Acharya NR, Doan T, Shantha JG.. Acute neuroretinitis as a delayed manifestation of tubulointerstitial nephritis and uveitis syndrome. Am J Ophthalmol Case Rep. 2024;34:102050. doi:10.1016/j.ajoc.2024.102050. PMID:38665419; PMCID:PMC11043875.