Optic nerve sheath meningioma (ONSM) is a tumor arising from the meninges that form the sheath of the optic nerve. It is relatively rare among orbital tumors, accounting for about 1-2% of all meningiomas, about 10% of all orbital tumors, and about 33% of optic nerve tumors. It occurs mostly in adults, particularly middle-aged women.
There are two main types of occurrence: the primary intraorbital type, which arises directly from the optic nerve sheath within the orbit, and the intracranial extension type, where a meningioma originating intracranially extends into the orbit via the optic canal. Distinguishing between these two types is important for determining management strategy.
There are several histological types of the tumor, broadly classified into the following three types.
Meningothelial type: Most common. Characterized by whorl formation.
Fibrous type: Proliferation of spindle-shaped cells.
Transitional type: Intermediate findings between the above two types.
It has been reported that about 20% of all cases show malignant features (cellular atypia, increased mitosis, necrosis, etc.). Most are classified as WHO Grade I (benign), but Grade II (atypical) and Grade III (malignant) also exist.
QIs optic nerve sheath meningioma malignant?
A
Most are benign (WHO Grade I), but about 20% have been reported to show malignant features. Rarely, they exhibit invasive or malignant characteristics and may have a higher recurrence rate. In children, the risk of malignant transformation and intracranial extension is higher compared to adults.
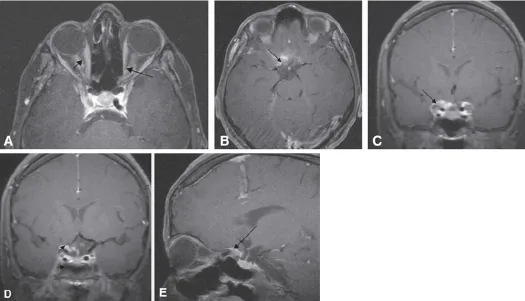
Badr MA, et al. Bilateral Optic Nerve Sheath Meningioma with Intracanalicular and Intracranial Component in a 25-year-old Saudi Patient. Middle East Afr J Ophthalmol. 2008;15(3):138-141. Figure 2. PMCID: PMC3040919. License: CC BY.
Contrast-enhanced T1-weighted axial MRI shows linear enhancement along the left optic nerve sheath (black arrows) running on both sides of the optic nerve, indicating the tram-track sign (Panel A); Panels B–E are coronal and sagittal images showing intracranial extension. This corresponds to the tram-track sign discussed in the section “2. Main Symptoms and Clinical Findings.”
The most characteristic symptom is slowly progressive unilateral vision loss, which follows a chronic course over months to years. Pain is usually absent.
Vision loss: The most common complaint. It progresses over years, and visual acuity at initial presentation varies.
Visual field defects: Various patterns including central sensitivity loss, concentric visual field constriction, and paracentral scotomas.
Proptosis: Mild proptosis may occur as the tumor enlarges.
Ocular motility disturbance: Mild restriction of eye movement may occur when the tumor is large.
As the tumor enlarges, fundus findings change as follows.
Early stage: Optic disc edema (reflecting impaired optic nerve blood flow due to the tumor).
After long-term course: Disc edema decreases and progresses to optic atrophy (pallor of the optic disc).
Optociliary shunt vessels: Collateral vessels seen around the optic disc, representing compensatory vascular formation in response to chronic compression of the central retinal vein by the tumor. They are known as one of the characteristic fundus findings in ONSM.
Passes through the optic disc margin and shows a large diameter
Imaging is most important for confirming ONSM, and the following patterns are known.
Main imaging patterns on CT/contrast-enhanced MRI:
Pattern
Features
Tubular type (tram-track sign)
Cylindrical enlargement along the entire optic nerve with double-line enhancement
Globular type
Spherically surrounds the optic nerve like an apple on an arrow
Eccentric type
Aneurysmal deviation and enlargement on one side of the optic nerve
Part of the tumor may contain calcifications (CT is superior for detection). On contrast-enhanced MRI, the tumor shows homogeneous and strong enhancement.
QWhat is the tram-track sign?
A
The tram-track sign is a characteristic imaging finding on axial contrast-enhanced CT or MRI, where the tumor appears as two linear (tram-track-like) shadows on both sides of the optic nerve. This occurs because the tumor grows around the optic nerve while the nerve itself is preserved. It is highly specific for ONSM, and in typical cases, imaging diagnosis is possible without biopsy.
ONSM is a relatively rare disease among orbital tumors.
Accounts for approximately 1–2% of all meningiomas
Seen in about 10% of all orbital tumors and about 33% of optic nerve tumors
Peak age of onset is 40–60 years (middle age)
More common in women (female:male ratio approximately 3:1)
Association with neurofibromatosis type 2 (NF2): NF2 is known as a hereditary condition associated with ONSM. The NF2 gene is located on the long arm of chromosome 22 (22q12) and encodes the merlin protein. Loss of merlin function is thought to be involved in tumor development. In pediatric ONSM cases, the rate of NF2 association is high, and attention should be paid to the risk of bilateral and multiple meningiomas.
In addition, exposure to ionizing radiation has been reported as a risk factor for meningiomas in general.
T2-weighted: Signal similar to fat (differentiating point from optic nerve glioma)
Post-contrast: Homogeneous and strong enhancement
Tram-track sign / doughnut sign (tumor encircles the optic nerve on coronal view)
Essential for evaluating intracranial extension
CT: CT is superior for detecting calcification. Tram-track sign can also be seen on CT. If the lesion extends to the optic canal, optic canal enlargement may be observed.
Fundus examination, visual field test, OCT: Used to evaluate optic disc morphology, optociliary shunt vessels, and retinal nerve fiber layer (RNFL) thickness. Visual field test helps identify the pattern of damage.
Common in children and associated with NF1. T2 hyperintense, uniform enlargement and tortuosity (downward kinking) of the optic nerve. Enhancement is mild to variable.
Optic neuritis
Acute or subacute vision loss. Pain (eye movement pain) present. Contrast-enhanced MRI shows enhancement within the optic nerve.
Acute or subacute course. Inflammatory thickening of the optic nerve sheath.
Lymphoma
Consider orbital infiltration of systemic lymphoma. Confirmed by tissue examination.
If NF2 is suspected, perform a detailed examination for bilateral vestibular schwannomas and multiple meningiomas.
Biopsy principle: If typical imaging findings (e.g., tram-track sign) are present, biopsy is usually unnecessary. The optic nerve and ONSM share pial blood flow, and surgical procedures including biopsy carry a high risk of damaging the optic nerve. If useful vision remains, surgical intervention should be avoided. 6)
QWhat is the difference from optic glioma?
A
Optic glioma is more common in children and is characteristically associated with NF1 (neurofibromatosis type 1), whereas optic nerve sheath meningioma occurs predominantly in middle-aged women and is known to be associated with NF2. On imaging, glioma shows uniform enlargement and tortuosity (downward kinking) of the optic nerve, with high signal on T2-weighted images. In contrast, optic nerve sheath meningioma shows enhancement of the optic nerve sheath (peripheral part) with a tram-track sign, and the optic nerve axons are preserved internally, which is a major distinguishing feature.
When visual function deterioration progresses or the tumor extends intracranially, stereotactic radiotherapy is the first choice. It is expected to preserve visual function and suppress tumor growth. 2)3)
Fractionated Stereotactic Radiotherapy (fSRT)
Fractionated stereotactic radiotherapy: Has the advantage of reducing damage to the optic nerve.
Dose: 50-54 Gy in 25-30 fractions is standard. Visual field stabilization/improvement rates of 83-100% have been reported. 3)5)
Gamma Knife (GKRS)
Stereotactic radiosurgery: Single fraction allows steep dose fall-off.
Tumor control rate of over 90% has been reported. Dose concentration is advantageous for exophytic tumors. 1)
CyberKnife
Robot-assisted stereotactic irradiation: Can treat tumors with complex shapes.
Tumor control rates equivalent to Gamma Knife have been reported. 4)
After radiotherapy, visual function preservation rates are 70-95%, and tumor control rates are over 90%. 2)3) Patients with better pre-treatment visual acuity have a better prognosis.
If useful vision remains, surgical resection is generally not recommended. The tumor and optic nerve share pial blood supply, so the risk of vision loss from resection is very high.
Cases where surgery may be considered:
In cases of complete blindness with severe proptosis and cosmetic deformity
When the tumor extends intracranially with risk of involvement of the contralateral optic nerve or optic chiasm
Progressive intracranial extension type that does not respond to conservative treatment (radiation therapy)
For intracranial extension, consider a combination of craniotomy and radiation therapy in collaboration with neurosurgery.
ONSM arises from the meninges (especially arachnoid cap cells) that form the optic nerve sheath. The optic nerve extends from behind the eye through the optic canal into the cranium, and is enveloped by a sheath consisting of dura mater, arachnoid mater, and pia mater along its entire length. The tumor originates from cells of this sheath and grows concentrically around the optic nerve.
NF2 gene (22q12): Encodes the merlin protein, which is involved in suppressing cell proliferation. Loss-of-function mutations lead to loss of tumor suppressor function, resulting in the development of meningiomas.
Immunohistochemistry: Positive for EMA, PR (progesterone receptor), and SSTR2A are characteristic. Ki-67 is low (2–3%) in Grade I.
WHO classification: The majority are Grade I (benign). Malignancy increases stepwise: Grade II (atypical, 4–19 mitoses/10 HPF + brain invasion, etc.), Grade III (malignant, ≥20 mitoses/10 HPF).
The tumor extends along the optic nerve sheath and compresses the optic nerve from the outside. This leads to visual impairment through the following pathways.
Direct compression: Mechanical compression and stretching of optic nerve axons.
Blood flow disturbance: Ischemia of optic nerve axons due to compression of pial vessels.
Central vein occlusion: Chronic compression of the central retinal vein → papilledema → formation of optociliary shunt vessels.
When the tumor is confined to the orbit, the prognosis for life is good, but if it extends into the optic canal or intracranially, it can affect the contralateral visual pathway and optic chiasm, worsening the prognosis.
ONSM is a benign tumor, and its natural course is characterized by slow progression over several years to decades.
Orbital confined type: Good prognosis for life. However, without treatment, vision gradually declines and may eventually lead to blindness.
After stereotactic radiotherapy: International reports indicate visual preservation rates of 70–95% and tumor control rates of over 90% 2)3).
Intracranial extension type: If it spreads to the contralateral optic nerve or optic chiasm, bilateral visual impairment may occur, leading to a poor prognosis.
NF2-associated type: There is a risk of multiple meningiomas, and long-term follow-up is essential.
After treatment, regular MRI, visual field, and visual acuity tests are performed to monitor for regrowth.
Proton beam radiotherapy: It is expected to reduce late toxicity due to low scatter dose. Especially in pediatric cases, it may be considered as an option from the perspective of reducing the risk of secondary cancer. 7)
Somatostatin receptor imaging (Ga-68 PET/CT): Meningiomas highly express somatostatin receptor (SSTR2A). Its application for evaluating tumor activity using functional imaging is being studied.
Mifepristone (antiprogesterone drug): As a drug therapy focusing on PR positivity in meningiomas, its use in refractory cases is being studied, but it is not established as standard treatment. 4)
Turbin RE, Thompson CR, Kennerdell JS, Cockerham KP, Kupersmith MJ.. A long-term visual outcome comparison in patients with optic nerve sheath meningioma managed with observation, surgery, radiotherapy, or surgery and radiotherapy. Ophthalmology. 2002;109(5):890-9; discussion 899-900. doi:10.1016/s0161-6420(02)01017-5. PMID:11986093.
Saeed P, Rootman J, Nugent RA, White VA, MacKenzie IR, Koornneef L. Optic nerve sheath meningiomas. Ophthalmology. 2003;110(10):2019-2030. doi:10.1016/s0161-6420(03)00787-5.
David W. Andrews, Rod Faroozan, Benson P. Yang, Richard S. Hudes, Maria Werner-Wasik, Sung M. Kim, Robert C. Sergott, Peter J. Savino, et al. Fractionated Stereotactic Radiotherapy for the Treatment of Optic Nerve Sheath Meningiomas: Preliminary Observations of 33 Optic Nerves in 30 Patients with Historical Comparison to Observation with or without Prior Surgery. Neurosurgery. 2002;51(4):890-904. doi:10.1227/00006123-200210000-00007.