The representative ocular side effects of steroid use (glucocorticoids) are posterior subcapsular cataract (PSC) and intraocular pressure elevation (steroid-induced glaucoma). They can occur with any route of administration: systemic, topical eye drops, inhalation, or topical skin application.
Posterior subcapsular cataract is the most common drug-induced lens opacity. Once it develops, it can cause severe visual impairment in a relatively short period.
There is individual variation in steroid-induced intraocular pressure elevation. When steroid eye drops are applied to normal eyes, about 35% show moderate pressure elevation (6–15 mmHg) and about 5% show severe elevation (≥15 mmHg) 1). In patients with primary open-angle glaucoma (POAG), the rate of high responders is markedly high at 46–92% 1).
Regarding the risk of PSC from inhaled steroids, an odds ratio (OR) increase of 1.3–1.5 has been reported with long-term high-dose use 2). For oral steroids, long-term use also increases the risk of open-angle glaucoma3).
Posterior subcapsular cataract: the most common drug-induced lens opacity
Intraocular pressure elevation due to steroid eye drops: approximately 35% moderate, approximately 5% severe 1)
Risk exists for all routes of administration (oral, eye drops, inhalation, topical, intravitreal injection)
Inhaled steroids also increase PSC risk (OR 1.3–1.5) 2)
QWill I definitely develop cataracts or glaucoma if I use steroids?
A
Not everyone develops these conditions. The risk of onset varies greatly depending on dose, duration, and individual susceptibility. Intraocular pressure elevation occurs in about 35% of patients (moderate, 6–15 mmHg) and about 5% (severe, 15 mmHg or more). Posterior subcapsular cataract is relatively rare with prednisolone-equivalent doses of 10 mg/day or less, but becomes more likely with high doses continued for more than one year. If long-term use is anticipated, regular ophthalmologic check-ups are recommended.
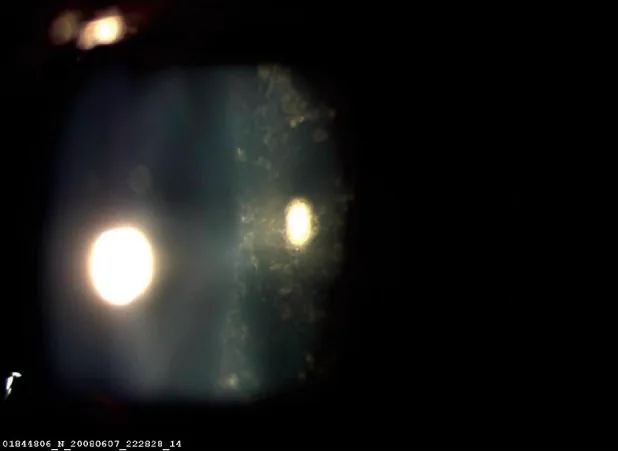
Chuang LH, et al. Ocular adnexal and ocular trauma imaging. Indian J Ophthalmol. 2009 Nov-Dec;57(6):470-472. Figure 1. PMCID: PMC2812771. License: CC BY.
Slit-lamp microscope image showing opacity of posterior subcapsular cataract (PSC) directly beneath the posterior capsule of the right eye. This corresponds to the typical opacity pattern of steroidcataract discussed in the section “Main symptoms and clinical findings.”
Ocular side effects of steroids present different symptoms and findings for cataracts and glaucoma.
Findings of steroid cataract (posterior subcapsular cataract)
Opacity pattern: Develops as faint punctate opacities or vacuoles directly beneath the posterior capsule on the visual axis
Progression pattern: Punctate opacities gradually coalesce into a well-demarcated, homogeneous, disc-shaped posterior subcapsular opacity (PSC)
Threshold for visual impairment: When the diameter of the posterior subcapsular opacity reaches 2 mm or more, visual impairment occurs and surgery is often required
Subjective symptoms: Primarily photophobia (glare), blurred vision, and decreased visual acuity. PSC is characterized by particularly poor vision in bright light when the pupil constricts
Findings of steroid glaucoma
Elevated intraocular pressure: Usually rises above 21 mmHg
Persistence of elevated intraocular pressure: The duration until normalization is proportional to the treatment period. For triamcinolone, it persists for 9 to 12 months
Diagnosis confirmed: If intraocular pressure normalizes after discontinuing steroids, the diagnosis is confirmed
Progressive findings: Persistent elevation of intraocular pressure leads to glaucomatous visual field defects (e.g., arcuate scotoma, nasal step)
QHow does steroid cataract affect vision?
A
Due to posterior subcapsular opacity, photophobia (glare) and blurred vision are common. Since PSC occurs just beneath the posterior capsule of the visual axis, visual acuity tends to decrease during the daytime or in bright environments when the pupil constricts, leading to a characteristic complaint of poorer vision during the day than at night. When the opacity diameter reaches 2 mm or more, visual impairment often interferes with daily activities.
The intraocular pressure-elevating effect of eye drops is proportional to their anti-inflammatory potency. The order of strength of intraocular pressure elevation is dexamethasone ≥ betamethasone > fluorometholone6), and a dose-dependent effect is observed.
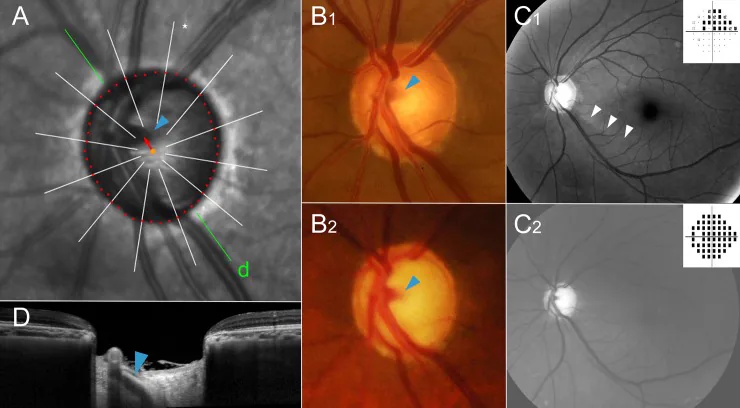
Lee KM, Kim M, Oh S, et al. Hemisphere opposite to vascular trunk deviation is earlier affected by glaucomatous damage in myopic high-tension glaucoma. PLoS One. 2020;15(5):e0233270. Figure 4. PMID: 32421695; PMCID: PMC7233594; DOI: 10.1371/journal.pone.0233270. License: CC BY.
Composite image showing infrared fundus image, optic disc photograph, OCT, and Humphrey visual field of a glaucoma case with a recorded maximum intraocular pressure of 36 mmHg. Corresponds to the evaluation of optic disc cupping, RNFL thinning, and visual field defects discussed in the section “Diagnosis and examination methods”.
QHow long does it take for steroid eye drops to raise eye pressure?
A
In some cases, an increase in eye pressure can be observed as early as 1–2 weeks after starting treatment. Stronger steroids such as dexamethasone are more likely to raise eye pressure, so regular eye pressure checks are necessary. Measurement of eye pressure 2–4 weeks after starting treatment is recommended. Fluorometholone has a weaker effect on raising eye pressure compared to dexamethasone and betamethasone, and may be used as an alternative in patients at high risk of increased eye pressure.
When dense opacification occurs in the posterior subcapsular region on the visual axis and the diameter of the posterior subcapsular opacity reaches 2 mm or more, visual impairment often occurs and surgery is often required.
The standard surgical procedure is phacoemulsification (PEA) with intraocular lens (IOL) implantation
If steroids are continued, the opacity may progress, so consider reducing or discontinuing the dose if possible
If continued steroid use is necessary for management of the underlying disease, regular follow-up should be performed even after cataract surgery
First step: Reduction or discontinuation of steroids
Reduce or discontinue steroids as much as possible. This may be difficult depending on the status of the underlying disease (e.g., collagen disease, kidney transplant). Consider switching to an alternative drug with a lower risk of increasing eye pressure (e.g., fluorometholone eye drops) 6).
Second stage: Conservative therapy with intraocular pressure-lowering medications
Depending on the level of visual impairment and intraocular pressure, the following are used as appropriate:
Prostaglandin (PG) analog eye drops
Beta-blocker eye drops
Carbonic anhydrase inhibitor (CAI) eye drops
Oral carbonic anhydrase inhibitor (acetazolamide): for acute intraocular pressure elevation
Management of residual triamcinolone
If intraocular pressure remains elevated after intravitreal injection, removal of residual triamcinolone from the vitreous (vitrectomy) or excision of the sub-Tenon triamcinolone depot may be effective.
Surgical treatment
Surgery is chosen when drug control is poor, visual impairment is progressing, and one cannot wait for intraocular pressure to decrease with steroid reduction or discontinuation.
Trabeculotomy is recommended as the first choice7)
Reasons include that patients are often young, the procedure is safe with few complications, and postoperative management is easy.
Trabeculectomy is a second-line option because of the high risk of scarring in young patients7)
QCan steroid-induced glaucoma be cured?
A
In many cases, intraocular pressure normalizes after discontinuing steroids. However, intraocular pressure elevation following intravitreal injection of triamcinolone may persist for 9 to 12 months. If high intraocular pressure continues for a long time, damage to the optic nerve and visual field becomes irreversible, so early intervention is important. When intraocular pressure control is poor with medication, trabeculotomy is effective, and particularly good results have been reported in young patients.
Steroids act directly on cells of the trabecular meshwork (the drainage pathway for aqueous humor) and increase resistance to aqueous outflow through multiple mechanisms.
Increased production of extracellular matrix (collagen, glycosaminoglycans, fibronectin, etc.) by trabecular meshwork cells, leading to narrowing of the meshwork structure 8)
Decreased phagocytic activity (debris removal function) of trabecular meshwork cells, resulting in accumulation of debris in the meshwork 8)
Steroid-induced expression of the myocilin (MYOC) gene leads to accumulation of abnormal protein in the trabecular meshwork8)
These changes accumulate, increasing resistance to aqueous outflow and elevating intraocular pressure
The above mechanisms are similar to those of primary open-angle glaucoma (POAG), and this is considered one reason why POAG patients are more likely to be high responders to steroids.
Metabolic abnormalities, membrane dysfunction, and oxidative damage caused by steroids impair lens transparency 9)
Formation of protein adducts and mechanisms mediated by glucocorticoid receptors are involved 9)
Abnormalities in cell adhesion molecules of lens epithelial cells occur
Decreased activity of Na-K ATPase (sodium-potassium pump) disrupts the ion and water balance in the lens, leading to opacification under the posterior capsule9)
The reason steroid-induced cataracts are more likely to occur in children is thought to be that lens epithelial cells during the growth period are more susceptible to the effects of steroids.
Development of selective glucocorticoid receptor modulators (SEGRMs): Research is progressing on drugs that maintain anti-inflammatory effects while reducing side effects10).
Intraocular pressure management with dexamethasone sustained-release implant (intravitreal): Elevated intraocular pressure occurs in about 30% of cases after administration, but it has been shown that most can be controlled with eye drops5).
General advances in MIGS (minimally invasive glaucoma surgery): New-generation surgeries that lower intraocular pressure with minimal invasiveness, such as iStent, Trabectome, Hydrus, and GATT, are being studied11).
Genetic polymorphisms and steroid sensitivity: Associations between polymorphisms in the MYOC gene and glucocorticoid receptor (GR) gene and high responders are being studied, and future personalized prediction is expected8).
Reduction of ocular side effects by steroid replacement therapy: Early switching to immunosuppressive drugs (cyclosporine, tacrolimus, etc.) may reduce steroid dosage and alleviate ocular side effects12).
Armaly MF. Statistical attributes of the steroid hypertensive response in the clinically normal eye. I. The demonstration of three levels of response. Invest Ophthalmol. 1965;4:187-197. PMID: 14283012.
Smeeth L, Boulis M, Hubbard R, Fletcher AE. A population based case-control study of cataract and inhaled corticosteroids. The British journal of ophthalmology. 2003;87(10):1247-51. doi:10.1136/bjo.87.10.1247. PMID:14507760; PMCID:PMC1920769.
Garbe E, LeLorier J, Boivin JF, et al. Risk of ocular hypertension or open-angle glaucoma in elderly patients on oral glucocorticoids. Lancet. 1997;350(9083):979-982. doi:10.1016/s0140-6736(97)03392-8.
Jones R 3rd, Rhee DJ. Corticosteroid-induced ocular hypertension and glaucoma: a brief review and update of the literature. Curr Opin Ophthalmol. 2006;17(2):163-7. doi:10.1097/01.icu.0000193079.55240.18. PMID:16552251.
Haller JA, Bandello F, Belfort R, Blumenkranz MS, Gillies M, Heier J, Loewenstein A, Yoon YH, Jiao J, Li XY, Whitcup SM, Ozurdex GENEVA Study Group, Li J.. Dexamethasone intravitreal implant in patients with macular edema related to branch or central retinal vein occlusion twelve-month study results. Ophthalmology. 2011;118(12):2453-2460. doi:10.1016/j.ophtha.2011.05.014. PMID:21764136.
Cantrill HL, Palmberg PF, Zink HA, Waltman SR, Podos SM, Becker B. Comparison of in vitro potency of corticosteroids with ability to raise intraocular pressure. American journal of ophthalmology. 1975;79(6):1012-7. doi:10.1016/0002-9394(75)90687-x. PMID:1173539.
Iwao K, Inatani M, Tanihara H, Japanese Steroid-Induced Glaucoma Multicenter Study Group. Success rates of trabeculotomy for steroid-induced glaucoma: a comparative, multicenter, retrospective cohort study. American journal of ophthalmology. 2011;151(6):1047-1056.e1. doi:10.1016/j.ajo.2010.11.028. PMID:21396622.
Clark AF, Wordinger RJ. The role of steroids in outflow resistance. Experimental eye research. 2009;88(4):752-9. doi:10.1016/j.exer.2008.10.004. PMID:18977348.
Jobling AI, Augusteyn RC. What causes steroid cataracts? A review of steroid-induced posterior subcapsular cataracts. Clinical & experimental optometry. 2002;85(2):61-75. doi:10.1111/j.1444-0938.2002.tb03011.x. PMID:11952401.
Sundahl N, Bridelance J, Libert C, De Bosscher K, Beck IM. Selective glucocorticoid receptor modulation: New directions with non-steroidal scaffolds. Pharmacology & therapeutics. 2015;152:28-41. doi:10.1016/j.pharmthera.2015.05.001. PMID:25958032.
Richter GM, Coleman AL. Minimally invasive glaucoma surgery: current status and future prospects. Clinical ophthalmology (Auckland, N.Z.). 2016;10:189-206. doi:10.2147/OPTH.S80490. PMID:26869753; PMCID:PMC4734795.
Jabs DA, Rosenbaum JT, Foster CS, Holland GN, Jaffe GJ, Louie JS, Nussenblatt RB, Stiehm ER, et al. Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders: recommendations of an expert panel. American journal of ophthalmology. 2000;130(4):492-513. doi:10.1016/s0002-9394(00)00659-0. PMID:11024423.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.