Age-related decline in visual acuity, contrast sensitivity, dark adaptation, stereopsis, and visual field that affects ADL, QOL, and fall risk is called “age-related visual function decline.” This visual decline is not merely “difficulty seeing” but is a major contributor to the deterioration of physical, mental, and social health in older adults (frailty).
Frailty refers to a state of vulnerability in older adults. In the phenotypic model proposed by Fried et al. (Fried criteria), meeting three or more of the following five items defines frailty, and one to two items defines prefrailty 1).
Weight loss: Unintentional loss of 4.5 kg or more per year, or 5% or more of body weight.
Fatigue: Subjective symptom of feeling “everything is a bother”
Decreased physical activity: Walking and other activities less than 150 kcal per week
Slowed walking speed: Usual walking speed less than 0.8 m/s
Decreased grip strength: Less than 26 kg for men, less than 18 kg for women
Relationship between visual impairment and frailty
Older adults with visual impairment are reported to have a 2 to 3 times higher risk of frailty compared to healthy individuals2). Decreased visual function is not just a local problem of “difficulty seeing” but becomes an entry point to frailty by triggering a chain of falls, avoidance of going out, social isolation, and cognitive decline.
The prevalence of visual impairment increases sharply after age 75. Visual impairment is established as an independent risk factor for falls3), and RCT data show that first-eye cataract surgery reduces fall risk by 34%3).
QIs age-related vision loss inevitable?
A
Presbyopia (loss of accommodation) begins around age 40 due to hardening of the lens, and progression is inevitable. However, visual function can be compensated with reading glasses, progressive lenses, or multifocal contact lenses. Vision loss due to cataracts can also be significantly improved by phacoemulsification and intraocular lens implantation, which is also expected to reduce fall risk. In many cases, the problem is not the decline in visual function itself but the lack of appropriate correction or treatment.
2. Symptoms of age-related visual function changes
Age-related visual function changes are classified into seven main categories.
Presbyopia (loss of accommodation)
Difficulty reading close-up text: The lens loses elasticity, making it hard to focus on near objects.
Holding smartphones farther away: Increased tendency to extend arms to see clearly at close range.
Slower reading speed: Eye strain easily occurs during prolonged near work.
Decreased contrast sensitivity and glare
Difficulty noticing steps and obstacles: Difficulty identifying objects in low-contrast environments.
Poor vision at night or on cloudy days: Scattered light and reduced sensitivity combine to decrease visual clarity.
Oncoming headlights are dazzling: Increased glare due to scattered light from cataracts.
Delayed dark adaptation and color vision changes
Difficulty walking in dark places: Slower regeneration of rhodopsin in rod cells, leading to delayed dark adaptation.
Changes in color perception: Yellowing of the lens reduces sensitivity to short wavelengths (blue), making it difficult to distinguish white and blue colors.
Visual field narrowing and reduced stereopsis
Overlooking peripheral obstacles: Visual field narrowing due to conditions like glaucoma reduces peripheral vision.
Difficulty judging distances: Reduced binocular vision accuracy leads to poorer stereopsis, making it hard to judge step height.
Tripping on stairs: Combined effects of reduced stereopsis and contrast sensitivity increase fall risk.
Visual impairment alone does not directly cause frailty, but it can lead to physical and social frailty through the following chain.
Falls and fractures: Visual impairment is an independent risk factor for falls3)
Avoidance of going out → Decreased physical activity → Sarcopenia (loss of muscle mass): Avoiding going out due to visual impairment reduces walking and exercise, leading to muscle weakness5)
Social isolation → depression and cognitive decline: Sensory impairments in vision and hearing have been reported to be significantly associated with depression and anxiety6)
QWhy does vision loss increase the risk of falls?
A
Two visual functions are important for preventing falls: recognizing steps and maintaining balance. When contrast sensitivity declines, low-contrast steps become harder to see; visual field loss leads to overlooking peripheral obstacles; and reduced stereopsis impairs judgment of step depth and height. The combination of these three visual impairments significantly increases fall risk.
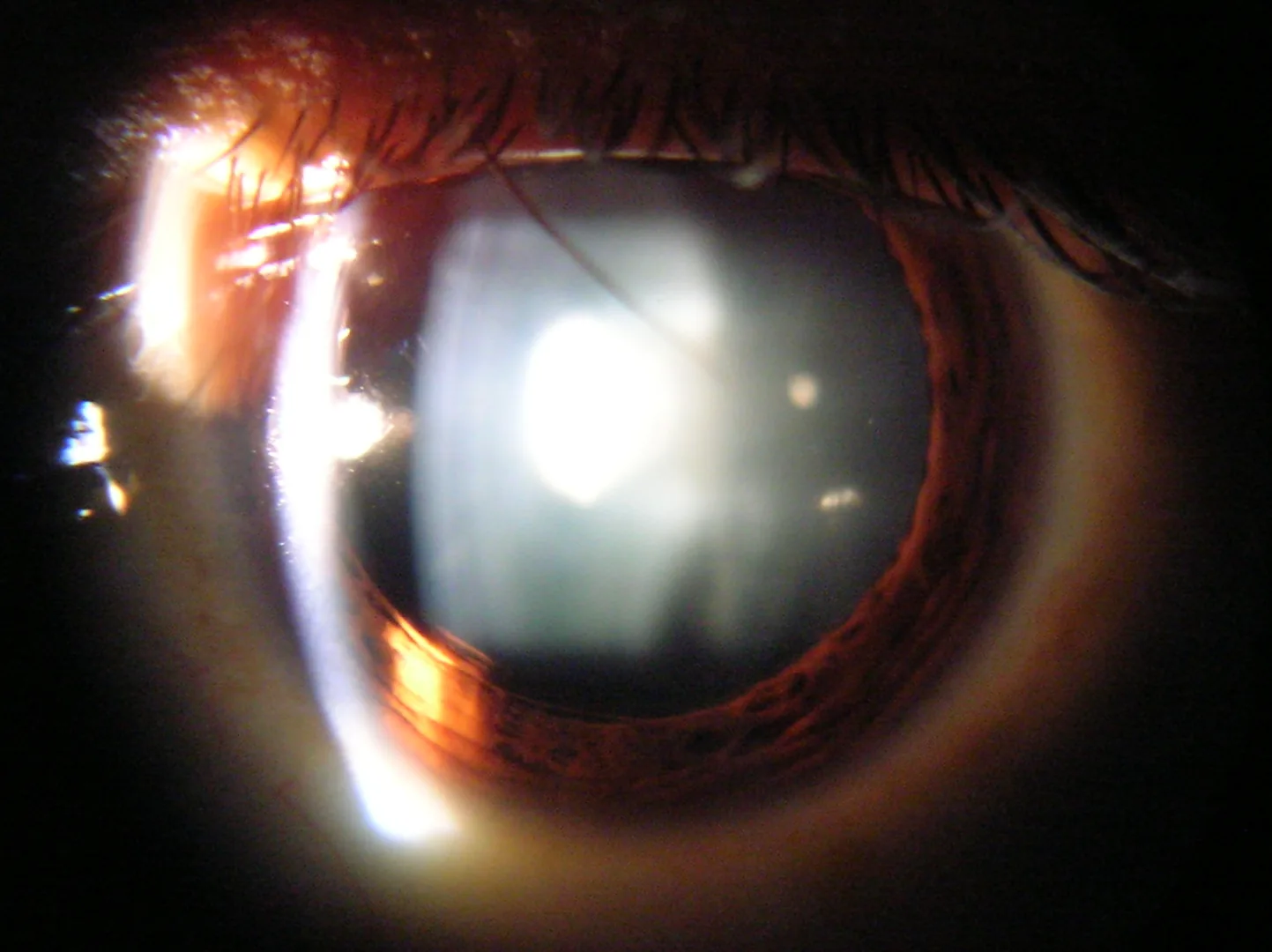
Ahuja R. Slit lamp view of cataract in human eye. 2005. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Slit_lamp_view_of_Cataract_in_Human_Eye.png. License: CC BY-SA 3.0.
Anterior segment photograph of a cataractous eye taken with a slit-lamp biomicroscope, showing whitening and light scattering due to opacification from the nucleus to the cortex of the lens. This corresponds to cataract (decreased contrast sensitivity and increased glare due to lens opacification) discussed in the section “Causes of Age-Related Visual Decline.”
Age-related visual decline involves a combination of local ocular structural changes and systemic age-related changes in neural function.
Cause of presbyopia: Accommodative power declines linearly from around age 40 due to nuclear sclerosis and loss of elasticity of the lens, as well as decreased function of the ciliary muscle7)
Cataract (opacification): Denaturation and aggregation of lens proteins (crystallins) increase scattered light, leading to decreased contrast sensitivity and increased glare8)
Glaucoma: Loss of retinal ganglion cells causes progressive visual field loss. Visual field defects often progress without noticeable symptoms, so early detection through health checkups is important9)
Age-related macular degeneration (AMD): Caused by age-related changes in the retinal pigment epithelium (RPE) and Bruch’s membrane, leading to significant central vision loss. The Hisayama study reported a 9-year incidence of new AMD of 4.8%10)
Delayed dark adaptation: Due to decreased density of retinal rod cells and slowed regeneration of rhodopsin (visual pigment)
Dry eye (decreased tear production): Meibomian gland dysfunction (MGD) and decreased tear secretion with age cause fluctuating visual function
Decreased visual processing speed: The information processing capacity of the cerebral cortex declines with age, prolonging visual reaction time15)
Vicious cycle of frailty: Malnutrition → muscle weakness → decreased physical activity → further malnutrition forms a vicious cycle1). Visual impairment can trigger this cycle
4. Visual Function Assessment and Frailty Screening
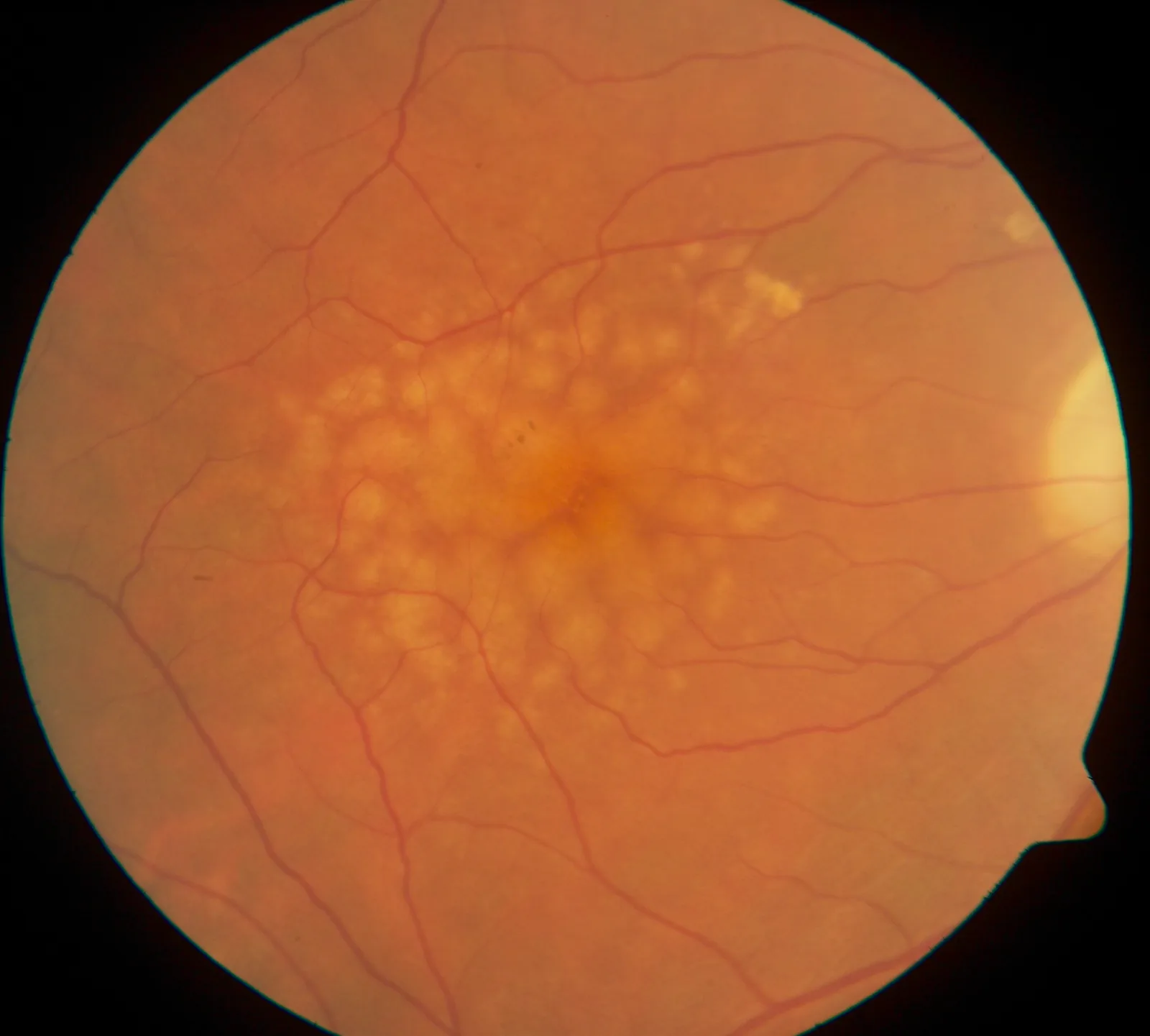
Ipoliker. Fundus image of macular soft drusen, right eye of a 70-year-old male. 2008. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Macular_Soft_Drusen.jpg. License: CC BY-SA 3.0.
Right eye fundus photograph of a 70-year-old male, showing numerous pale yellow to white soft drusen scattered mainly in the macula. This corresponds to early findings of age-related macular degeneration (AMD) discussed in the section “Visual Function Assessment and Frailty Screening.”
Assessment of visual impairment and frailty is performed by combining ophthalmological and systemic evaluations.
The Pelli-Robson chart measures contrast sensitivity by varying the contrast of letters in steps, and can detect decreased contrast sensitivity even when visual acuity is within the normal range11).
The VFQ-25 (25-Item National Eye Institute Visual Function Questionnaire) is a 25-item questionnaire that assesses the impact of visual function on daily life, and is widely used as a patient-reported outcome measure for a broad range of eye diseases including cataract, glaucoma, and AMD13).
The Ministry of Health, Labour and Welfare’s Basic Checklist is a screening tool for preventing the need for long-term care, consisting of 25 items related to exercise, nutrition, oral health, going out, forgetfulness, and depression12). Combining it with ophthalmic visual function assessment makes it easier to detect declines in daily functioning associated with visual impairment.
QHow can I know if I am frail?
A
It is recommended to combine screening by a primary care physician using the Ministry of Health, Labour and Welfare’s Basic Checklist with ophthalmic visual function assessment (visual acuity, contrast sensitivity, visual field testing). If 8 or more items on the Basic Checklist are positive, the risk of needing long-term care is considered high. When visual impairment is identified, interventions to improve visual function such as cataract surgery, refractive correction, and low vision care are the first steps in preventing falls and frailty.
5. Countermeasures and Prevention (Visual Function Correction, Frailty Prevention)
Jeannin S. Expérimentation sur les risques de chute des personnes âgées avec le LBMC. 2022. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Exp%C3%A9rimentation_sur_les_risques_de_chute_des_personnes_%C3%A2g%C3%A9es_avec_le_LBMC.jpg. License: CC BY-SA 4.0.
Photo of a fall risk assessment experiment for older adults at the LBMC Biomechanics Laboratory, where a dual-task evaluation combining balance measurement and cognitive tasks is being conducted. This corresponds to the fall risk reduction and physical function assessment discussed in the section “Countermeasures and Prevention (Visual Function Correction, Frailty Prevention).”
Treatment by Visual Function Disease and Frailty Prevention Effects
Improve lighting: Keep the illuminance of living rooms and hallways at 300 lux or higher to compensate for reduced contrast sensitivity and reduce fall risk.
Contrast tape: Apply to the nosing of stairs to make steps easier to recognize for older adults with visual field loss or reduced contrast sensitivity.
Non-slip mats: Place in wet areas such as bathrooms and washrooms to reduce fall risk.
Active exercise prescription after vision correction is effective for frailty prevention. Walking and balance training (e.g., tai chi, yoga) have been reported to reduce fall risk 3). Improving visual function increases the frequency of going out, and promoting social participation helps prevent sarcopenia (muscle loss) and cognitive decline 5).
QDoes cataract surgery reduce fall risk?
A
Yes, it does. In a randomized controlled trial (RCT) by Harwood et al., older women who underwent first-eye cataract surgery had a 34% reduction in fall risk 3). In a second-eye surgery RCT by Foss et al., visual function and health status improved, but the 32% reduction in fall rate was not statistically significant, and the effect was considered uncertain 4).
6. Physiological Background of Age-Related Changes
With aging, the lens undergoes nuclear sclerosis, yellowing, and loss of elasticity 8). Nuclear sclerosis results from oxidation and cross-linking of crystallin proteins, leading to increased light scattering (glare and reduced contrast) and loss of accommodative power (presbyopia). Yellowing increases absorption of short-wavelength light, manifesting as reduced blue color perception.
Age-related decline in meibomian gland function (MGD) and atrophy of lacrimal glands reduce the quality and quantity of tears 7). This destabilizes the tear film, causing fluctuations in visual function. Dry eye has a high prevalence among older adults and is a major cause of visual variability.
The density of rod cells (photoreceptors for night and scotopic vision) decreases with age, and the regeneration rate of rhodopsin (visual pigment) slows. This prolongs dark adaptation (adjustment from bright to dark environments), making nighttime walking difficult. Cone cells (photoreceptors for daytime and color vision) are also affected by aging, leading to reduced high-frequency contrast sensitivity.
Visual processing speed from the retina to the visual cortex (occipital lobe) declines with age 15). The time required for the brain to process signals from the eyes (visual reaction time) increases, making it difficult to respond quickly to moving objects. This is also associated with fall risk.
The vicious cycle of frailty is formed as “malnutrition → muscle weakness → reduced activity → further malnutrition” 1). Visual impairment intervenes in this cycle through multiple pathways. Reduced physical activity due to avoidance of going out leads to sarcopenia (loss of skeletal muscle mass and strength), increasing the risk of falls, fractures, and subsequent bedridden state. Visual impairment is also a strong predictor of social frailty 2).
Cataract surgery and cognitive function: A nationwide cohort study in Taiwan by Tsai et al. reported a significant reduction in the risk of dementia among older adults who underwent cataract surgery 16), suggesting that improvement in visual function may contribute to cognitive protection.
AI-assisted visual function assessment: Fundus image analysis using machine learning and deep learning has advanced, leading to early detection of AMD, diabetic retinopathy, and glaucoma, as well as improved efficiency in screening for visual impairment.
Evolution of multifocal intraocular lenses: Recent multifocal and extended depth of focus (EDOF) intraocular lenses have improved presbyopia correction after cataract surgery, significantly reducing dependence on glasses postoperatively.
Integration of ophthalmic assessment into community-based integrated care: Efforts have begun to incorporate ophthalmic visual function evaluation into the comprehensive frailty assessment process for older adults. The linkage between the Ministry of Health, Labour and Welfare’s basic checklist and ophthalmic screening is recognized as a challenge in community-based integrated care12).
Development of low vision care systems: The Japan Ophthalmologists Association’s Smart Site related information includes leaflets that connect to consultation desks and low vision care facilities in each region, which can be used for collaboration between eye clinics and local support organizations14).
Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. The journals of gerontology. Series A, Biological sciences and medical sciences. 2001;56(3):M146-56. doi:10.1093/gerona/56.3.m146. PMID:11253156.
Swenor BK, Lee MJ, Varadaraj V, et al. Aging with vision loss and its impact on physical, cognitive, psychological, and social outcomes. Annu Rev Vis Sci. 2020;6:161-180.
Harwood RH, Foss AJ, Osborn F, et al. Falls and health status in elderly women following first eye cataract surgery: a randomised controlled trial. Br J Ophthalmol. 2005;89(1):53-59. doi:10.1136/bjo.2004.049478.
Foss AJ, Harwood RH, Osborn F, Gregson RM, Zaman A, Masud T. Falls and health status in elderly women following second eye cataract surgery: a randomised controlled trial. Age and ageing. 2006;35(1):66-71. doi:10.1093/ageing/afj005. PMID:16364936.
Chen SP, Bhattacharya J, Bhattacharya S. Multi-dimensional impact of serious eye disease in older adults. Am J Ophthalmol. 2014;157(3):686-693.
Cosh S, von Hanno T, Helmer C, Bertelsen G, Delcourt C, Schirmer H, et al. The association amongst visual, hearing, and dual sensory loss with depression and anxiety over 6 years: The Tromsø Study. International journal of geriatric psychiatry. 2018;33(4):598-605. doi:10.1002/gps.4827. PMID:29193338.
Andersen GJ. Aging and vision: changes in function and performance from optics to perception. Wiley Interdiscip Rev Cogn Sci. 2012 May-Jun;3(3):403-410. doi:10.1002/wcs.1167. PMID:22919436; PMCID:PMC3424001.
Asbell PA, Dualan I, Mindel J, Brocks D, Ahmad M, Epstein S. Age-related cataract. Lancet. 2005;365(9459):599-609. doi:10.1016/S0140-6736(05)17911-2.
Yasuda M, Kiyohara Y, Hata Y, et al. Nine-year incidence and risk factors for age-related macular degeneration in a defined Japanese population: the Hisayama Study. Ophthalmology. 2009;116(11):2135-2140. doi:10.1016/j.ophtha.2009.04.017. PMID:19744734.
Pelli DG, Robson JG, Wilkins AJ. The design of a new letter chart for measuring contrast sensitivity. Clin Vis Sci. 1988;2(3):187-199.
Mangione CM, Lee PP, Gutierrez PR, Spritzer K, Berry S, Hays RD, National Eye Institute Visual Function Questionnaire Field Test Investigators. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol. 2001;119(7):1050-1058. doi:10.1001/archopht.119.7.1050. PMID:11448327.