Oculomotor synkinesis, also called aberrant regeneration or misdirection of the third cranial nerve (oculomotor nerve), is a condition in which firing of the oculomotor nerve causes paradoxical simultaneous contraction of muscles other than the intended target. “Synkinesis” refers to involuntary muscle contractions that occur with voluntary movements.
The oculomotor nerve innervates the inferior oblique, medial rectus, superior rectus, inferior rectus, pupillary sphincter, and levator palpebrae superioris muscles. Its nucleus is located in the midbrain tegmentum, runs ventrally between the posterior cerebral artery and superior cerebellar artery, and enters the lateral wall of the cavernous sinus. Parasympathetic fibers run in the dorsomedial aspect of the nerve’s outermost layer and divide into superior and inferior branches at the superior orbital fissure.
The incidence of aberrant regeneration after acute oculomotor nerve injury is reported to be approximately 15% 1). In congenital oculomotor nerve palsy, aberrant regeneration is observed in 61–93% of cases.
Experiments on cat sciatic nerves in 1928 and Bielschowsky’s description in 1935 established the phenomenon of “regenerating nerve fibers growing into incorrect sheaths.”
QCan synkinesis occur after oculomotor nerve palsy due to diabetes or hypertension?
A
It usually does not occur. Ischemic oculomotor nerve palsy is neurapraxia (a conduction block that preserves axonal continuity) and does not involve neurotmesis (nerve severance), which is a prerequisite for aberrant regeneration. See the “Pathophysiology” section for details.
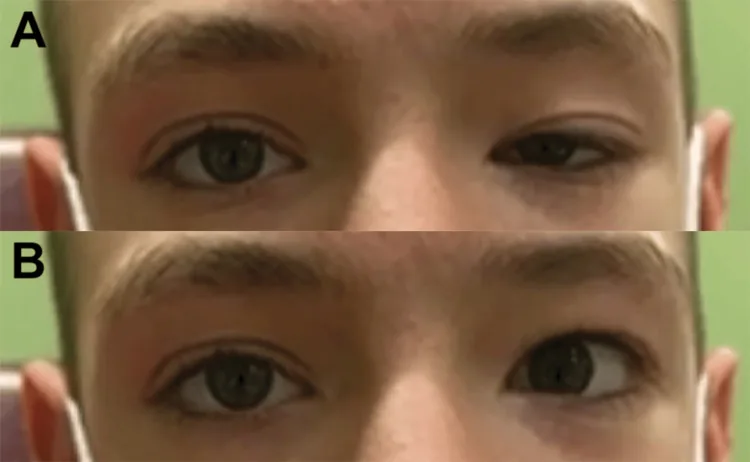
Report of a Rare Case and Literature Review of Combined Marcus Gunn Jaw Winking Synkinesis and Monocular Elevation Deficiency. Cureus. 2025 Jul 16; 17(7):e88119. Figure 1. PMCID: PMC12267604. License: CC BY.
Preoperative evaluation of MGJWS Image A was taken at rest. Image B was taken during active jaw movement. MGJWS: Marcus-Gunn jaw winking synkinesis
Signs of third cranial nerve palsy: Ptosis of the affected eye. Partial or complete paralysis of muscles innervated by the third cranial nerve. Pupil may or may not be involved.
Pseudo Von-Graefe Sign: Elevation of the upper eyelid on downward gaze or adduction. This occurs because nerve fibers that normally innervate the medial rectus and inferior rectus muscles abnormally innervate the levator palpebrae superioris muscle1)2).
Abnormal adduction: Adduction occurs when attempting upward or downward gaze.
Globe retraction and movement restriction: Limitation of elevation and depression accompanied by retraction of the globe when attempting vertical movements.
Inverse Duane Sign: Globe retraction and narrowing of the palpebral fissure during abduction2).
Pseudo-Argyll Robertson Pupil: Pupillary constriction on near response is more prominent than the light reflex, and eye movement-induced pupillary constriction is observed2).
QWhat is the pseudo Von-Graefe sign?
A
This is a sign where the upper eyelid of the affected eye paradoxically elevates during downward gaze and adduction. It occurs due to aberrant regeneration of the oculomotor nerve, where fibers destined for the medial rectus and inferior rectus muscles come to innervate the levator palpebrae superioris muscle1)2). It is one of the most characteristic findings of oculomotor synkinesis.
Cavernous sinus thrombosis (CST): Also reported in children2).
Meningocele: Compression by a meningocele in the oculomotor cistern. Association with idiopathic intracranial hypertension (IIH) has been suggested1).
Tumor: Parasellar tumors, etc.
Onset timing: Appears weeks to months after acute palsy.
Primary (rare)
Slowly progressive lesions in the cavernous sinus: Synkinesis occurs without preceding obvious oculomotor nerve palsy.
Meningioma: Slow compression within the cavernous sinus.
Cavernous sinus aneurysm: Aneurysm within the cavernous sinus.
Schwannoma: Schwannoma within the cavernous sinus.
Mechanism: Ephaptic transmission (electrical crosstalk between nerve fibers due to myelin damage) is considered a contributing factor.
Other rare causes include ophthalmoplegic migraine, Tolosa-Hunt syndrome, and Miller-Fisher syndrome.
The frequency of causes of oculomotor nerve palsy in adults is approximately 20% each for aneurysm and ischemia, 15% for tumors, and 10% for trauma. In children, congenital causes account for 43–47%, trauma 13–23%, tumors 10%, and aneurysms 7%.
QWhat is the difference between primary and secondary oculomotor synkinesis?
A
Secondary synkinesis occurs weeks to months after acute oculomotor nerve palsy due to aberrant regeneration. Primary synkinesis occurs without preceding obvious palsy and is often caused by slowly progressive lesions in the cavernous sinus (meningioma, aneurysm, schwannoma).
Clinical diagnosis based on medical history and physical examination is fundamental. Confirmation of a “reproducible pattern of synkinetic movements” is key.
Important history: history of oculomotor nerve injury such as traumatic brain injury or neurosurgery. Course of acute-onset diplopia and ptosis that partially resolved spontaneously.
Ophthalmic and neurological examination: sensorimotor examination, assessment of ptosis and anisocoria, pupillary response in light and dark, fundus examination (for optic disc edema or optic atrophy).
The ice test (applying an ice pack to the upper eyelid for 2 minutes → improvement of ≥2 mm is positive, sensitivity 80–92%) is useful for differentiating myasthenia gravis.
Ischemic oculomotor nerve palsy (usually no synkinesis): Often resolves spontaneously within 1–3 months. Oral vitamin B complex and circulation-improving drugs are used.
Inflammatory (Tolosa-Hunt syndrome): Prednisone® 50–60 mg/day for 3 days, then taper while monitoring for recurrence.
Traumatic: Recovery is relatively difficult. If no improvement after 6 months, consider strabismus surgery or levator advancement.
Cavernous sinus thrombosis (CST): Acute management with systemic antibiotics plus anticoagulants (enoxaparin). Synkinesis may persist afterward2).
Strabismus surgery planning must account for aberrant regeneration (synkinesis). Surgery on the non-paretic eye (contralateral eye) is recommended, with a combination of large lateral rectus recession and small medial rectus resection. The use of adjustable sutures is useful2).
QIs strabismus surgery possible in patients with oculomotor nerve synkinesis?
A
It is possible, but a surgical plan that accounts for aberrant regeneration is necessary. Shortening of the ipsilateral medial rectus should be avoided, and surgery on the non-paralyzed eye (lateral rectus recession + medial rectus resection) is recommended2). Surgery is often planned in two stages, and adjustable sutures are frequently used.
After nerve transection, regenerating axons enter endoneurial tubes different from their original ones and innervate different muscles. As a result, firing of a single nerve fiber causes simultaneous contraction of multiple muscles.
In primary oculomotor synkinesis, “ephaptic transmission” is also discussed as a mechanism. Demyelination due to slowly progressive lesions in the cavernous sinus may cause electrical crosstalk between individual nerve fibers.
In idiopathic intracranial hypertension (IIH), cerebrospinal fluid is redistributed as a compensatory mechanism based on the Monro-Kellie hypothesis (constant intracranial volume: brain tissue, CSF, blood). This results in optic nerve sheath distension, empty sella, transverse sinus stenosis, and meningocele formation. There is a pathway in which a meningocele in the oculomotor cistern compresses the oculomotor nerve, leading to paralysis and then synkinesis1). Up to 10% of IIH patients have a meningocele.
Molecular mechanisms of congenital oculomotor synkinesis
A homozygous missense mutation in the chemokine receptor ACKR3 (CXCR7) has been identified in humans, causing isolated oculomotor synkinesis presenting with ptosis and ipsilateral eyelid elevation on abduction. ACKR3 binds CXCL12 (also a ligand for CXCR4). Eyelid retraction in Duane retraction syndrome is also considered a form of oculomotor synkinesis.
7. Latest research and future perspectives (research-stage reports)
Walker et al. (2026) reported a 29-year-old man with oculomotor nerve palsy and synkinesis caused by a meningocele of the oculomotor cistern 1). Imaging findings of IIH (empty sella, transverse sinus stenosis, optic nerve sheath distention and tortuosity, BMI >40) were retrospectively identified. CISS sequence revealed the meningocele and oculomotor nerve atrophy. Symptoms improved mildly over 5 months then plateaued, with persistent movement limitation and diplopia. Although up to 10% of IIH patients have meningoceles, this is the first reported case of an oculomotor cistern meningocele causing synkinesis.
Oculomotor Synkinesis After Pediatric Cavernous Sinus Thrombosis (2021)
Lalwani et al. (2021) reported a 4-year-old boy 2). The course progressed from pustule at the nasal tip → ethmoid sinusitis → left orbital cellulitis → cavernous sinus and superior ophthalmic vein thrombosis. Eye movements improved with vancomycin + ceftazidime (IV antibiotics) and enoxaparin (anticoagulation), but 6 months after treatment, pseudo-von Graefe sign, inverse Duane sign, and pseudo-Argyll Robertson pupil appeared. Oculomotor synkinesis secondary to pediatric foveal retinal thickness is very rare.
ACKR3 (CXCR7) mutations have been identified in humans (Whitman et al. 2019), and three mouse models have been reported. Future genetic functional analysis is expected to elucidate the mechanisms of congenital malformations.
Walker B, Modi KA, Freitas LF, Shekhrajka N. Oculomotor Synkinesis Secondary to Meningocele: Report of a Rare Case. The Indian journal of radiology & imaging. 2026;36(1):128-131. doi:10.1055/s-0045-1810018. PMID:41523346; PMCID:PMC12788922.
Lalwani S, Kekunnaya R, Sheth J. Oculomotor synkinesis: an uncommon sequela of paediatric cavernous sinus thrombosis. BMJ Case Rep. 2021;14:e239819.