Ligneous conjunctivitis is an extremely rare conjunctivitis characterized by chronic, recurrent formation of a woody hard fibrinous pseudomembrane on the palpebral conjunctiva. The name “ligneous” (wood-like) derives from the characteristic hardness of this pseudomembrane.
This disease is strongly associated with type I plasminogen deficiency (hypoplasminogenemia). Plasminogen is the precursor of the fibrinolytic enzyme plasmin. Its quantitative or functional deficiency prevents fibrin dissolution, leading to accumulation as a pseudomembrane. The estimated prevalence is 1.6 per million people 2)4). As of 2001, fewer than 120 cases had been reported in the past 50 years.
Mutations in the PLG gene are the cause, with an autosomal recessive inheritance pattern. Onset often occurs in infancy, but adult-onset cases have also been reported 1). Pseudomembranous lesions may involve systemic mucous membranes such as gums, ears, airways, female genitalia, and kidneys. Co-occurrence with congenital hydrocephalus has also been reported 2)4)5).
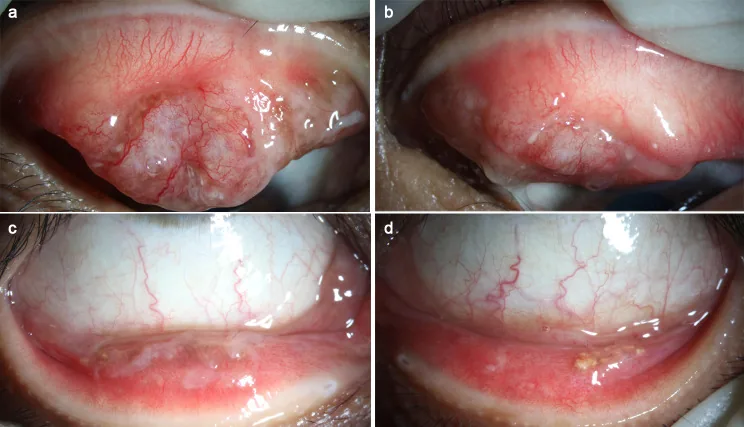
Jing Li, Rui Liu, Tingting Ren, Hong Zhang, et al. A case of IgG4-positive ligneous conjunctivitis mistaken for a conjunctival mass 2023 Jun 29 Diagn Pathol. 2023 Jun 29; 18:77 Figure 1. PMCID: PMC10308656. License: CC BY.
In A and C, thick yellowish-white pseudomembranes adhere to the upper palpebral conjunctiva with dilation of superficial vessels. In B and D, similar yellowish-white deposits are seen on the lower palpebral conjunctiva, with lesions spreading to both upper and lower conjunctiva.
Viscous discharge, hyperemia, and foreign body sensation appear as initial symptoms. Lacrimation may also occur. It may precede or coincide with systemic infections (upper respiratory tract infections, ear infections, etc.).
Pseudomembrane of the palpebral conjunctiva: A hard, thick, yellowish-white pseudomembrane commonly occurs on the upper eyelid. It recurs even after removal.
Often bilateral: Approximately 50% of cases are bilateral, and after the upper eyelid, it occurs on the lower eyelid and bulbar conjunctiva.
Corneal complications: Long-term inflammation can lead to corneal opacity, neovascularization, and corneal perforation.
Eyelid induration: The eyelid may become hard due to pseudomembrane formation.
Systemic Findings
Gingivitis and gingival lesions: The second most common site of involvement after the conjunctiva.
Airway lesions: Pseudomembranes can form in the larynx, vocal cords, and tracheobronchial tree. Airway obstruction is life-threatening 2).
Congenital hydrocephalus: Thought to be caused by obstruction of the ventricular system due to fibrin deposition 2)4)5).
Others: Pseudomembrane formation may also occur in the female genitalia, kidneys, and middle ear.
Histologically, eosinophilic amyloid-like material containing fibrin and immunoglobulins is found beneath the ulcerated conjunctival epithelium, with infiltration of lymphocytes, plasma cells, and neutrophils 1). Very rarely, IgG4-positive findings are observed, and there have been reports of misdiagnosis as conjunctival tumor 1).
Li et al. reported a case of ligneous conjunctivitis in a 41-year-old woman referred for bilateral conjunctival tumors. Pathological examination showed IgG4-positive findings (IgG4+ cells ≈ 100/HPF, IgG4/IgG ratio > 40%), suggesting that inflammation in LC may trigger immune abnormalities leading to elevated IgG4. After surgical excision and topical steroid administration, the patient remained recurrence-free for 10 months. 1)
QIs it a disease only in children?
A
Ligneous conjunctivitis often occurs in infants, but it can also occur in adults and the elderly. Cases have been reported where treatment was first received at ages 46 and 70. It is a disease that can occur across a wide age range.
The main cause of ligneous conjunctivitis is type I plasminogen deficiency due to mutations in the PLG gene.
There are two types of plasminogen deficiency. In type I (hypoplasminogenemia), both the antigen level and activity of plasminogen are reduced. In type II (dysplasminogenemia), the antigen level is normal but functional activity is decreased 3). Ligneous conjunctivitis is mainly associated with type I.
Genetic factors: Various mutations in the PLG gene have been reported, such as c.2095T>C (p.Cys699Arg) 2), c.2287C>T (p.Pro763Ser) 4), and c.1752-1753insG (p.Cys585ValfsX15) 5).
Consanguinity: Because it is an autosomal recessive disorder, consanguineous marriage is a risk factor 1)2)4)5). It is reported to be more common in populations from the Middle East and Turkey 4).
Tranexamic acid: It can induce ligneous conjunctivitis through inhibition of plasmin. Discontinuation may lead to improvement.
Trauma/Infection: External irritation to the conjunctiva triggers the wound healing cascade, leading to pseudomembrane formation.
There is no established consensus on curative treatment for ligneous conjunctivitis. The basic approach is a combination of surgical excision and pharmacotherapy.
Pharmacotherapy
Steroid eye drops: Basic treatment for suppressing inflammation. Long-term use requires caution for steroid-induced glaucoma.
Cyclosporine eye drops: Suppresses pseudomembrane recurrence through immunosuppression 4)
Heparin eye drops: Directly inhibits fibrin production 3)
Plasminogen eye drops: Promotes local fibrinolysis. Not commercially available in many regions.
Systemic therapy and others
Fresh frozen plasma (FFP): Local or systemic administration of plasma containing plasminogen 3)5)
Cryo-depleted plasma: Plasma from which coagulation factors have been removed from FFP. Can supplement plasminogen while reducing thrombotic risk 4)
Ryplazim: Human-derived plasminogen preparation. FDA-approved for the treatment of type I PLGD.
Pseudomembrane excision: When performed alone, it can reform within 48 hours, so it must be combined with pharmacotherapy.
Almeida et al. reported that with a protocol of pseudomembrane excision + intraoperative subconjunctival FFP injection + postoperative topical FFP and heparin eye drops, two cases remained recurrence-free for 12 months 3).
Case 1 (46-year-old male) had a plasminogen level of 4.75 mg/dL, and had repeated recurrences with previous excision + autologous serum, cyclosporine, and tacrolimus. With the FFP + heparin protocol, no recurrence was observed for 12 months. Case 2 (70-year-old female) had plasminogen activity of 43%, and similarly remained recurrence-free with the same protocol. 3)
Bonde Scheel-Bech et al. reported a 12-year-old Turkish girl (PLG activity <10%) who received intravenous cryo-depleted plasma 2-3 times per week plus cyclosporine eye drops; the pseudomembrane resolved within 7 weeks, and complete remission was maintained at 1 year 4).
Cryo-depleted plasma is a preparation from which cryoprecipitate has been removed from FFP. It lacks procoagulant factors, thus reducing the risk of thrombosis, while retaining normal levels of plasminogen. Compared to FFP, it can be administered in larger volumes, offering the advantage of achieving higher blood plasminogen concentrations. 4)
QIs it not curable by simply excising the pseudomembrane?
A
Excision alone has a very high recurrence rate, with pseudomembrane reformation as early as within 48 hours. This is because the surgical trauma itself promotes fibrin deposition. Excision must always be combined with pharmacotherapy such as heparin eye drops or fresh frozen plasma.
The pathology of ligneous conjunctivitis is based on impairment of the fibrinolytic pathway of the plasminogen-plasmin system.
Normal wound healing process: Tissue injury → deposition of fibrin matrix → granulation tissue formation → fibrin degradation by plasmin → collagen remodeling → healing.
Pathogenesis of ligneous conjunctivitis:
PLG gene mutation reduces the production or function of plasminogen
Insufficient conversion of plasminogen to plasmin
Inability to adequately degrade fibrin on damaged mucosa
Accumulation of serofibrinous material, forming a fibrin-rich pseudomembrane
The pseudomembrane hardens, presenting a characteristic “wood-like” appearance
The conjunctiva is frequently exposed to stimuli such as dust, local infection, and minor trauma, especially in infants. This makes the conjunctiva the most commonly affected organ.
The complication of hydrocephalus is thought to be caused by obstruction of cerebrospinal fluid circulation due to fibrin deposition in the ventricular system 2)4)5). In one case series, hydrocephalus was observed in 7 out of 16 children with ligneous conjunctivitis 5).
Alghubaishi et al. reported a case of a full-term male infant with a homozygous mutation in the PLG gene (c.2095T>C, p.Cys699Arg) who presented with congenital hydrocephalus, ligneous conjunctivitis, and recurrent meningitis. Plasminogen levels were markedly reduced to 15% (normal 75-150%), and an intracardiac thrombus was also noted. Despite intensive care, the patient died of upper airway obstruction before 1 year of age. 2)
QDoes plasminogen deficiency affect organs other than the eyes?
A
Yes. Plasminogen deficiency causes systemic impairment of fibrinolysis. It can affect multiple organs, including gingivitis, pseudomembrane formation in the airways (risk of airway obstruction), female genital tract lesions, renal impairment, and congenital hydrocephalus. Airway lesions in particular can be life-threatening, and early diagnosis and multidisciplinary collaboration are important.
Ryplazim (human-derived plasminogen preparation): It is the first FDA-approved treatment for type I plasminogen deficiency. Intravenous administration can control systemic ligneous lesions. The recommended dose is 6.6 mg per kg body weight every 2 to 4 days. However, it is difficult to obtain in many regions and is expensive, posing challenges.
Efficacy of cryo-depleted plasma: Bonde Scheel-Bech et al. reported the efficacy of long-term administration of cryo-depleted plasma as an alternative to conventional FFP 4). By removing coagulation factors while retaining plasminogen, it allows large-volume administration with reduced thrombotic risk.
FFP-based treatment protocol: In resource-limited settings, FFP is gaining attention as a practical treatment option 5). Almeida et al. reported favorable long-term outcomes with a perioperative protocol of pseudomembrane excision plus FFP plus heparin 3).
Association with IgG4-related disease: There have been only two reports of IgG4 positivity in LC to date, suggesting that chronic inflammation in LC may trigger immune abnormalities 1). Further accumulation of cases is needed to elucidate the relationship between the two diseases.
Gene therapy: Gene therapy as a definitive treatment for the PLG gene is still in the research stage, but it is expected as a future therapeutic option.
Li J, Liu R, Ren T, Zhang H, Ma J. A case of IgG4-positive ligneous conjunctivitis mistaken for a conjunctival mass. Diagnostic pathology. 2023;18(1):77. doi:10.1186/s13000-023-01366-0. PMID:37386507; PMCID:PMC10308656.
Alghubaishi SA, Saeed M, Abujamous F, Osman H, Alasmari BG. Recurrent Meningitis and Its Rare Association With Ligneous Conjunctivitis and Congenital Plasminogen Deficiency. Cureus. 2023;15(9):e44813. doi:10.7759/cureus.44813. PMID:37818495; PMCID:PMC10561533.
Almeida SCGB, Marback PMF. Ligneous conjunctivitis: Fresh-frozen plasma and heparin use intra-and postoperatively, a report of two cases. Arquivos brasileiros de oftalmologia. 2024;87(3):e20220288. doi:10.5935/0004-2749.2022-0288. PMID:38537040; PMCID:PMC11627270.
Bonde Scheel-Bech A, Roed Rasmussen ML, Heegaard S, Schmidt IM, Stensballe J. Cryo-Depleted Plasma Infusions for Ligneous Conjunctivitis. Case reports in ophthalmology. 2025;16(1):542-550. doi:10.1159/000546953. PMID:40777150; PMCID:PMC12331225.
AboGhayyada I, Zeidan M, Makhlouf TZ, AbuGhiyatha A, Ghnimat M, Najajreh M. Fresh frozen plasma therapy in type I plasminogen deficiency: a case of ligneous conjunctivitis with hydrocephalus. Oxford medical case reports. 2025;2025(12):omaf260. doi:10.1093/omcr/omaf260. PMID:41458265; PMCID:PMC12741436.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.