Infectious crystalline keratopathy (ICK) was first reported as a case of non-inflammatory bacterial colonization in a corneal graft after penetrating keratoplasty, and its clinical importance has since been recognized 2). It is characterized by thin, branching, crystal-like opacities in the corneal stroma with minimal surrounding inflammation 1).
ICK most commonly occurs under topical immunosuppressive therapy (steroid eye drops) after corneal transplantation 3). It appears snowflake-like or ice-crystal-like and tends to occur near sutures or surgical wounds in the corneal stroma3). The number of ICK cases has increased with the rise in penetrating keratoplasty2).
ICK predominantly affects adults and is usually unilateral 2). No gender or racial predilection has been identified 2). The most common causative organism is Streptococcus mitis (viridans group streptococci), but Gram-negative bacteria, fungi, and Acanthamoeba have also been reported 1).
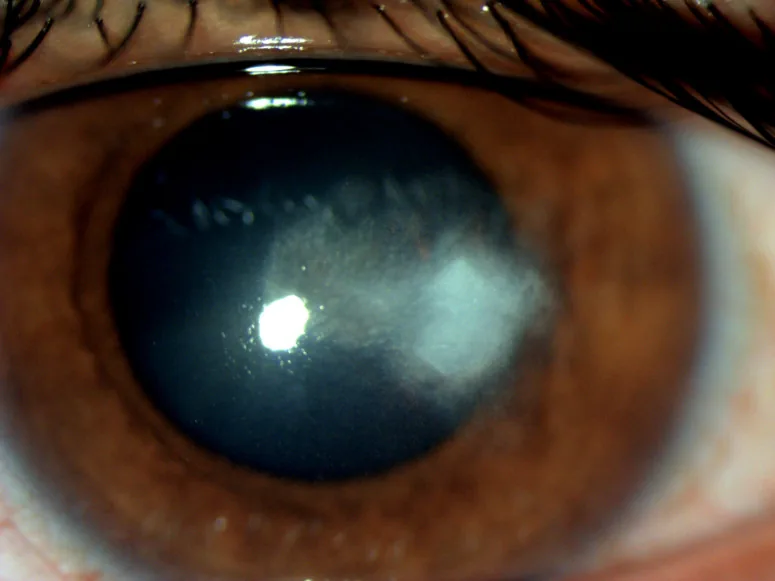
Zeba Khanam, Gaganjeet Singh Gujral, Shariq Wadood Khan Infectious crystalline keratitis induced by Citrobacter 2021 May 17 GMS Ophthalmol Cases. 2021 May 17; 11:Doc09 Figure 1. PMCID: PMC8167372. License: CC BY.
Needle-like, branching gray-white opacities with little inflammatory reaction spread within the corneal graft stroma. The crystalline infiltrates running through the graft represent the early stage of infectious crystalline keratopathy.
ICK may be asymptomatic 1). When symptoms occur, mild visual impairment is common 3). Photophobia and pain may also occur but are milder compared to other infectious keratitis 1). Under immunosuppression, local inflammation is suppressed, so patients may have few subjective symptoms, leading to delayed diagnosis 3).
Slit-lamp examination reveals branching, needle-like, or fern-like crystal-like opacities in the corneal stroma1)2). The opacities are often distributed in the anterior to mid-stroma 2). Conjunctival injection and anterior chamber inflammation are mild or absent, which is an important distinguishing feature from other infectious keratitis 1).
Corneal edema or epithelial defects are absent or minimal. Hypopyon is usually not observed. In corneal transplant eyes, lesions tend to occur at the graft-host junction and around sutures 3).
Even without immunosuppression, ICK can develop in neurotrophic corneal diseases (after herpetic keratitis, corneal surgery denervation, long-term topical anesthetic use) 1). The neurotrophic state delays corneal wound healing and provides an opportunity for initial pathogen colonization 1).
Many causative organisms of ICK form biofilms 1). Biofilms inhibit antibiotic penetration and are a major cause of treatment resistance 1). The minimum inhibitory concentration of streptococci cultured from ICK tends to be higher than when treating the same species in other situations, suggesting the influence of biofilms 1).
QWhat is a biofilm?
A
A biofilm is a protective film composed of a polysaccharide matrix produced by bacteria. By being encased in the biofilm, bacteria are protected from antimicrobial agents and immune cells. In ICK, the biofilm forms within the corneal stroma, so topical antibiotic eye drops alone cannot achieve sufficient drug concentration, making treatment difficult.
The diagnosis of ICK is based on characteristic clinical findings. Branching crystalline opacities and the absence of inflammation are key to diagnosis1)2).
Corneal scraping culture should be performed, but superficial scraping often fails to reach deep causative bacteria, resulting in negative results1)2). Corneal biopsy is useful to increase the culture positivity rate2). Corneal biopsy is taken from the edge of the infiltrate3).
Confocal microscopy can visualize highly reflective needle-like structures in the stroma and confirm the presence of crystalline keratopathy, but it is insufficient for identifying individual pathogens1).
Anterior segment OCT (AS-OCT) is useful for assessing the depth and extent of opacities and also aids in differential diagnosis2). AS-OCT can evaluate the distribution pattern of hyperreflective lesions localized to the subepithelial and anterior stroma2).
Differential Diagnosis of ICK
Paraproteinemic keratopathy: Bilateral and progressive. Caused by corneal deposition of immunoglobulin light chains. Confirm M protein by blood test2).
Corneal dystrophy: Check family history. Often occurs at a young age.
Drug-induced crystalline deposits: Check history of topical medications such as fluoroquinolones.
Cystinosis: A systemic metabolic disease that commonly occurs in children.
Gout: A systemic disease associated with elevated uric acid levels.
Key Points for Diagnosis
Absence of inflammation: The most characteristic feature of ICK is the near absence of hyperemia and anterior chamber inflammation.
Review of medical history: History of corneal transplantation, steroid use, or herpetic keratitis can provide diagnostic clues 2).
Bilateral cases: ICK is usually unilateral; in bilateral cases, consider non-infectious causes such as paraproteinemic keratopathy 2).
Limitations of culture: Superficial scrapings are often negative. Consider corneal biopsy 1).
QHow is ICK differentiated from paraproteinemic keratopathy?
A
ICK is usually unilateral with a history of corneal transplantation or steroid use. Paraproteinemic keratopathy progresses bilaterally and often has no ocular history. AS-OCT assessment of deposit depth and blood tests (free light chains, M protein) are useful for differentiation. Even with a typical ICK appearance, if there are no ocular risk factors or if it is bilateral, non-infectious causes should be actively investigated.
Initial treatment involves high-concentration broad-spectrum topical antibiotics. Frequent instillation of cefazolin (50 mg/mL) or vancomycin to cover Gram-positive bacteria, along with fluoroquinolones (e.g., moxifloxacin), is recommended 4). Once the causative organism is identified, treatment should be adjusted based on susceptibility 3).
Discontinuation or reduction of immunosuppressive therapy is a key component of treatment 3). Reducing steroid eye drops may unmask the inflammatory response contained within the biofilm, temporarily worsening symptoms 3).
Intrastromal antibiotic injection is an effective option for cases resistant to topical therapy 1). There are reports of ICK caused by Streptococcus mitis/parasanguinis treated with intrastromal cefuroxime 1), and two intrastromal injections of cefuroxime (1 mg/0.1 mL) and moxifloxacin (0.5 mg/0.1 mL) successfully treated ICK in a GVHD patient without therapeutic PK 1).
Intrastromal injection delivers antibiotics directly to the deep site of pathogens at high concentrations, overcoming the biofilm barrier. Injections should be performed in a circular pattern around the crystalline deposits, with the needle entry site away from the visual axis. 1)
If there is no response to antibiotic therapy or if severe corneal scarring remains, therapeutic full-thickness penetrating keratoplasty (PK) may be necessary 2)3).
QIs intrastromal antimicrobial injection safe?
A
Intrastromal injection uses drugs at concentrations similar to those used for intracameral injection during cataract surgery, so the risk of endothelial toxicity is considered low. It is important to limit the injection volume to prevent Descemet’s membrane detachment and to place the needle track outside the visual axis. It has been reported that no endothelial dysfunction or other signs of corneal toxicity were observed during follow-up of more than two years.
The pathogenesis of ICK begins with microbial entry into the corneal stroma through an epithelial defect 1). Microorganisms proliferate using the stromal lamellar spaces and the spaces between keratocyte cell bodies 1).
In an immunosuppressed state, the inflammatory response and immune cell infiltration are suppressed. Because the edema and purulent changes seen in typical infectious keratitis do not occur, a crystalline appearance forms 1). This characteristic appearance appears only with immunosuppression 1).
Biofilm formation is central to the pathology of ICK 1). The causative bacteria are protected within the biofilm, and the minimum inhibitory concentration for topical antimicrobials increases to four times or more than usual 1). Because the biofilm is located deep in the stroma, drug penetration from the surface is insufficient, leading to treatment resistance.
Long-term use of steroid eye drops increases the risk of ICK 3). In addition to local immunosuppression, corticosteroid-induced inhibition of collagen synthesis may also contribute to corneal weakening 3). Steroid eye drops are also commonly cited as a risk factor for fungal keratitis4).
QWhy is the inflammatory response minimal in ICK?
A
Many patients who develop ICK are receiving steroid eye drops after corneal transplantation or systemic immunosuppressive therapy. This immunosuppression suppresses inflammatory cell infiltration and the inflammatory response. Additionally, the biofilm inhibits immune cell access. As a result, the purulent changes and edema seen in typical infectious keratitis do not occur, and characteristic crystalline opacities form.
Intrastromal antimicrobial injection is gaining attention as a new treatment strategy for ICK 1). Compared to topical eye drops, it can deliver high concentrations of drugs directly to deep pathogens covered by biofilm 1). However, guidelines for drug selection, concentration, and injection volume have not been established, and future clinical trials are needed 1).
Paraproteinemic keratopathy can initially present as unilateral, subepithelial crystalline deposits similar to IKC. In crystalline keratopathy without a history of immunosuppression, progression to bilateral involvement should be monitored, and screening for M protein via blood tests is recommended. 2)
AS-OCT evaluation of the depth and distribution of corneal deposits has been reported to be useful in differential diagnosis 2). In differentiating IKC from non-infectious crystalline keratopathy (such as paraproteinemic keratopathy), establishing a systematic approach combining clinical findings, AS-OCT, and blood tests is a future challenge 2).
In the microbiological diagnosis of infectious keratitis, rapid identification by PCR of corneal scrapings is becoming practical 4). In conditions like IKC where culture-negative cases are common, the introduction of molecular biological methods may contribute to improved diagnostic accuracy.
Martinez-Velazquez L, Ma KK, Patel NS, Luo ZK. Successful Management of Infectious Crystalline Keratopathy with Intrastromal Antibiotic Injections. Case reports in ophthalmological medicine. 2022;2022:5830617. doi:10.1155/2022/5830617. PMID:36504920; PMCID:PMC9729021.
Aramburu-González A, López-Plandolit Antolin S, Márquez-Navarro JA. Paraproteinaemic keratopathy simulating a crystalline keratopathy. BMC ophthalmology. 2024;24(1):263. doi:10.1186/s12886-024-03487-6. PMID:38898421; PMCID:PMC11186065.
American Academy of Ophthalmology Cornea/External Disease Preferred Practice Pattern Panel. Bacterial Keratitis Preferred Practice Pattern. Ophthalmology. 2024.