내인성

진균성 안내염
한눈에 보는 포인트
섹션 제목: “한눈에 보는 포인트”1. 진균성 안내염이란?
섹션 제목: “1. 진균성 안내염이란?”진균성 안내염은 안내액(유리체, 전방수)에 진균이 감염 및 증식하는 중증 안질환입니다. 감염 경로에 따라 내인성(혈행성 파종)과 외인성(수술, 외상, 각막염으로부터의 전파)의 두 가지 유형으로 분류됩니다.
내인성 안내염의 절반 이상이 진균성이며, 30%가 양안성입니다. 외인성은 수술 후, 외상 후, 각막염 관련의 세 가지 범주로 세분됩니다7). 세균성 안내염에 비해 진행이 느리며, 수일에서 수주에 걸쳐 증상이 악화됩니다.
외인성
감염 경로: 수술, 외상, 각막염으로부터의 전파
주요 원인균: 아스페르길루스속 (가장 흔함)
빈도: 대부분 단안성
분류: 수술 후, 외상 후, 각막염 관련의 세 가지 범주
원인균은 Candida속·Aspergillus속이 대표적이지만, 희소 균종에 의한 보고도 증가하고 있습니다. Trichosporon속 (에키노칸딘계 약물에 자연 내성) 6), C. rugosa (비알비칸스 Candida의 0.1% 미만) 3), Arthrographis kalrae 5), Neoscytalidium dimidiatum 7) 등이 보고되었습니다.
COVID-19 유행 이후, 스테로이드 사용으로 인한 면역억제를 계기로 한 진균성 안내염이 잇따라 보고되고 있습니다 1, 9).
2. 주요 증상과 임상 소견
섹션 제목: “2. 주요 증상과 임상 소견”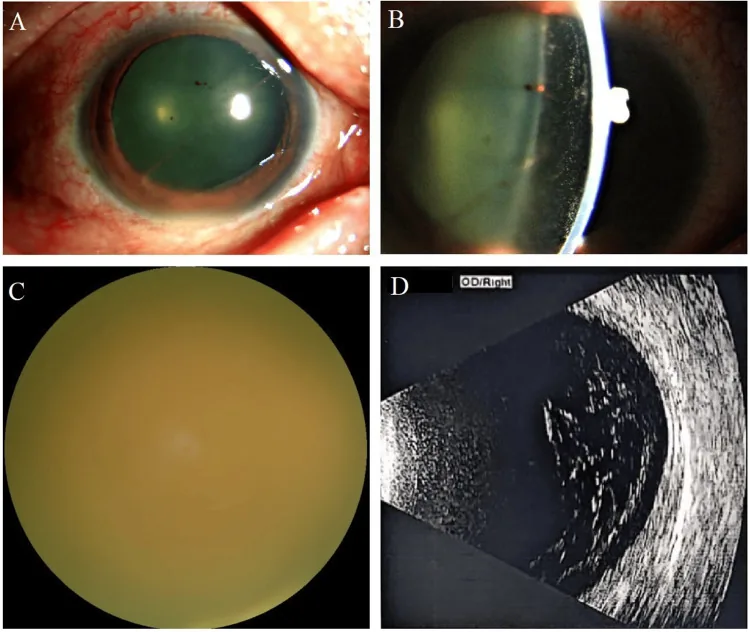
Nianjia Wang; Jiayi Wu; Xintong Xiang; Qian Zhao; Liang Yao. Endogenous Fungal Endophthalmitis Following Eyebrow Tattooing: A Case Report. Cureus.; 17(9):e93246. Published 2025. Figure 2. PMCID: PMC12553984. License: CC BY.
우안의 기저 안과 검사 소견. (A) 현저한 섬모체 충혈. (B) 세극등 검사에서 전방 내 다량의 염증 세포와 현저한 방수 플레어가 관찰됨. (C) 치밀한 유리체 혼탁으로 안저 관찰 불가. (D) 안구 B-초음파에서 광범위한 유리체 혼탁이 보임.
자각 증상
섹션 제목: “자각 증상”비문증, 안개시, 시력 저하가 초기 증상으로 흔합니다. 진행된 경우 안통, 충혈을 동반합니다.
원인균에 따라 병의 진행 속도가 다릅니다.
- 칸디다 안내염: 잠행성으로, 수일~수주에 걸쳐 시력이 저하됩니다.
- 아스페르길루스 안내염: 더 급성 경과를 취하며, 치밀한 유리체 혼탁을 동반하여 급속히 시력이 저하됩니다.
- 외인성 (수술 후·외상 후): 아급성
만성으로, 잠복기는 수주수개월에 이를 수 있습니다.
임상 소견
섹션 제목: “임상 소견”후극부를 중심으로 경계가 불명확한 황백색 솜털 모양의 맥락망막 침윤을 나타냅니다. 망막 내 출혈을 동반할 수 있습니다.
- 진균구 (fungus ball): 깃털 모양의 특징적인 유리체 혼탁. 칸디다 안내염에서 보입니다.
- 「진주 목걸이」양 소견: 국소 유리체 염증의 응집에 의한 염주 모양 혼탁. Klebsiella 감염과의 합병 예에서도 확인되었습니다 8).
- 오진 위험: 진균 감염이 수술 후 재발성 유리체염으로 간과되기 쉽습니다. 스테로이드 투여로 악화된 사례가 보고되었습니다4).
- 유육종증과의 유사성: 유리체 혼탁의 형태가 유사하여 초기에는 최대 50%에서 오진될 수 있습니다2).
Q
진균성 안내염의 증상은 다른 안과 질환과 구별하기 어렵습니까?
A
유리체 혼탁의 외관은 유육종증과 같은 비감염성 포도막염과 유사하며, 초기에는 최대 50%가 오진된다는 보고가 있습니다2). 또한 수술 후 재발성 유리체염으로 진균 감염을 간과하는 경우도 있습니다4). 자세한 내용은 「진단 및 검사 방법」 항목을 참조하십시오.
3. 원인 및 위험 요인
섹션 제목: “3. 원인 및 위험 요인”내인성과 외인성에 따라 위험 요인이 다릅니다. 주요 위험 요인은 다음과 같습니다.
| 분류 | 주요 위험 요인 |
|---|---|
| 내인성 | 중심정맥영양, 면역억제제, 스테로이드 |
| 내인성 | 장기 이식, 호중구 감소증, 악성 종양 |
| 내인성 | 당뇨병, 장기 ICU 입원 |
| 외인성 | 수술 중 합병증, 고령, 스테로이드 점안액 |
| 외인성 | 각막궤양, 콘택트렌즈 부적절 사용 |
COVID-19 관련 사례에서는 장기 입원과 전신 스테로이드 투여가 면역억제를 초래하여 진균성 안내염을 유발한 것으로 보고되었습니다1, 9). 유방암 화학요법(도세탁셀에 의한 백혈구 감소증)3), 면역억제 요법(메토트렉세이트 + 스테로이드)2), 콘택트렌즈 사용 중 위생 관리 불량으로 인한 각막염 파급5), IOL에 진균 바이오필름 정착6), 식물 외상에 의한 식물병원성 진균 감염7), 당뇨병 조절 불량4, 8)도 보고되었습니다.
Q
COVID-19 이후 진균성 안내염의 위험이 있습니까?
A
있습니다. COVID-19 치료에 사용되는 전신 스테로이드나 장기 ICU 입원이 면역억제를 초래하여 내인성 진균성 안내염의 유발 요인이 될 수 있습니다1, 9). 시력 변화가 발생하면 신속히 안과 진료가 필요합니다.
4. 진단 및 검사 방법
섹션 제목: “4. 진단 및 검사 방법”배양 및 미생물학적 검사
섹션 제목: “배양 및 미생물학적 검사”안내액 배양이 표준 검사입니다. 유리체 검체는 전방수보다 진단율이 높습니다. 배지는 사부로 한천 배지를 사용하며, 37°C와 실온 두 조건에서 최소 2주간 배양합니다.
혈액 배양은 내인성 증례의 1/3~1/2에서만 양성이므로, 음성이더라도 안내염을 배제할 수 없습니다.
증균 배양: 유리체액을 혈액 배양 병에 접종하면 평균 1.23일 만에 양성화되는 것으로 보고되었습니다6).
보조 진단
섹션 제목: “보조 진단”- β-D-글루칸: 보조 진단에 사용되지만 음성인 경우가 있습니다. C. rugosa 증례에서 혈청 ≤3.2 pg/mL, 유리체 ≤3.0 pg/mL로 낮은 값이 보고되었습니다 3).
- PCR(범진균 프라이머/ITS 유전자): 배양 음성에서도 균종 동정이 가능합니다. COVID-19 동반 증례 및 C. rugosa 증례에서 유용성이 보고되었습니다 1, 3).
- MALDI-TOF MS: 신속하고 정확한 균종 동정을 가능하게 합니다 6).
약제 감수성 검사
섹션 제목: “약제 감수성 검사”원인균이 확인되면 반드시 약제 감수성 검사를 시행합니다. Aspergillus terreus는 암포테리신 B에 높은 비율(98%)로 내성을 보입니다(MIC 2 μg/mL) 2). Trichosporon inkin의 플루코나졸 감수성(MIC 2.0 μg/mL)이 확인된 증례에서는 플루코나졸 단독 치료가 성공했습니다 6).
Q
혈액 검사가 음성이어도 진균성 안내염의 가능성이 있습니까?
A
있습니다. 내인성 안내염에서도 혈액 배양 양성은 1/3~1/2에 불과합니다. β-D-글루칸도 음성인 경우가 있습니다 3). 안내액의 직접 배양 및 PCR이 확진에 필수적입니다.
5. 표준 치료법
섹션 제목: “5. 표준 치료법”전신 투여
섹션 제목: “전신 투여”주요 항진균제의 특징은 아래와 같습니다.
| 약제 | 투여 경로 | 특징 |
|---|---|---|
| 플루코나졸 | 정맥/경구 | 칸디다 1차 선택 |
| 보리코나졸 | 정맥주사/경구 | 사상균 및 내성 칸디다에 효과적 |
| 암포테리신 B | 정맥주사/유리체내 | 광범위, 안내 침투성 제한적 |
- 플루코나졸: 정맥주사 100 mg 또는 경구 200~400 mg/일. 칸디다 맥락망막염의 1차 선택제.
- 보리코나졸: 사상균 및 플루코나졸 내성 칸디다에 효과적. 경구 200 mg/일. 유리체내 침투성이 우수함.
- 암포테리신 B: 광범위 스펙트럼이나 안내 침투성은 제한적. 신독성이 문제됨 2).
- 이사부코나졸: 보리코나졸 혈중 농도가 낮을 때 대체 약물로 보고됨 1, 2).
- 미카펀진: A. terreus 예에서 300 mg/일 사용이 보고됨 2). 그러나 Trichosporon 속에는 자연 내성이 있어 사용하지 않음 6).
치료 기간은 일반적으로 4~6주. Trichosporon inkin에서 플루코나졸 16주 투여로 억제 성공 사례가 있음 6).
유리체내 주사
섹션 제목: “유리체내 주사”- 암포테리신 B: 5 μg/0.1 mL 2).
- 보리코나졸: 100 μg. 유리체절제안에서 반감기는 약 8시간 (암포테리신 B는 24시간 이상) 2).
유리체절제술(PPV)
섹션 제목: “유리체절제술(PPV)”감염원의 물리적 제거(감량), 약물 확산 촉진, 검체 채취를 위해 시행합니다. 다음 경우에 적응됩니다.
- 유리체 혼탁이 심하여 약물 요법만으로는 불충분한 경우
- 확진을 위해 검체 채취가 필요한 경우
- 난치성 또는 재발성 사례
IOL 관련 증례에서는 IOL 및 생물막을 포함한 수정체낭 제거가 중요합니다5, 6).
원인균별 치료 전략
섹션 제목: “원인균별 치료 전략”칸디다
맥락망막염만 있는 경우: 경구 아졸계(플루코나졸, 보리코나졸)
유리체 침범이 있는 경우: 유리체절제술 + 유리체내 항진균제 주사 추가
치료 기간: 원칙적으로 4~6주
아스페르길루스
1차 선택: 보리코나졸(A. terreus는 암포테리신 B 내성률 98%)
국소 요법: 유리체절제술 + 유리체내 보리코나졸 주사
감수성 검사: 필수(내성 확인을 위해)
희소 균종
Trichosporon: 에키노칸딘 무효. 플루코나졸 감수성 확인 후 사용
기타: MALDI-TOF MS로 동정 후, 약제 감수성 검사에 기반하여 선택
Q
진균성 안내염에 스테로이드를 사용해서는 안 되는가?
6. 병태생리학·상세한 발병 기전
섹션 제목: “6. 병태생리학·상세한 발병 기전”내인성 안내염의 진행 과정
섹션 제목: “내인성 안내염의 진행 과정”진균혈증→맥락막·망막 정착→감염 병소 형성→유리체 파종→안내염→범포도막염→전안구염의 단계적 진행을 따른다.
- 아스페르길루스의 혈관 중심성 침입: 혈관 주변에서 침입하여 혈관 폐쇄와 출혈성 병변을 형성한다.
- IOL 바이오필름: 진균이 인공수정체(IOL)에 부착·증식하여 면역 회피 기전으로 기능한다. 이것이 만성·재발성 감염의 원인이 된다6).
희소 균종의 특수한 병태 기전
섹션 제목: “희소 균종의 특수한 병태 기전”Koide 등(2023)은 C. rugosa 안내염 1예를 보고하고 Virchow-Robin 공간을 통한 유리체강 내 침입 경로를 시사했습니다3). C. rugosa는 비알비칸스 칸디다 중 0.1% 미만의 희소 균종이지만 면역억제 상태에서는 침습성 감염을 일으킵니다.
Kaderli Tamer 등(2022)은 COVID-19 치료 중 발생한 안내염 증례에서 스테로이드가 혈액-망막 장벽 파괴를 강화하고 진균의 안내 침입을 촉진했다고 보고했습니다9).
Trichosporon 속은 협막 다당류(글루쿠로노자일로만난; GXM) 항원을 생성하여 식세포에 의한 식균 작용을 억제함으로써 침습성 감염을 성립시킵니다6). 이 기전은 에키노칸딘 계열 약물에 대한 자연 내성과 함께 난치성의 주된 원인입니다.
7. 최신 연구와 향후 전망(연구 단계 보고)
섹션 제목: “7. 최신 연구와 향후 전망(연구 단계 보고)”포비돈 요오드 관류 유리체 절제술
섹션 제목: “포비돈 요오드 관류 유리체 절제술”난치성 진균성 안내염에 대한 새로운 치료법으로 유리체 절제술 중 0.025% 포비돈 요오드를 관류액으로 사용하는 술기가 보고되었습니다.
Huang 등(2024)은 Arthrographis kalrae에 의한 중증 안내염 1예에 0.025% 포비돈 요오드 관류 유리체 절제술을 시행했습니다5). 기존 항진균제로 조절이 어려웠던 감염이 이 수술로 제압되었습니다. 포비돈 요오드는 내성 메커니즘이 없어 다제내성 진균에 대한 대책으로 기대됩니다.
신속 진단 기술의 발전
섹션 제목: “신속 진단 기술의 발전”- MALDI-TOF MS: 기존의 형태학적 동정이나 생화학적 동정보다 신속하고 정확한 균종 동정이 가능합니다6). Trichosporon inkin 등 희소 균종 동정에 특히 유용합니다.
- PCR + 시퀀싱: 배양 음성 증례에서도 ITS 유전자 영역을 표적으로 한 panfungal PCR로 균종 동정이 가능합니다1, 3). COVID-19 팬데믹 이후 혈액 배양 음성 내인성 안내염 증례의 진단에 기여하고 있습니다.
미해결 과제
섹션 제목: “미해결 과제”Trichosporon 속에 대한 항진균제의 브레이크포인트(임상적 한계점)는 아직 확립되지 않았습니다6). 각 시설의 약제 감수성 시험 결과에 기반한 개별 치료가 현재 상황이며, 근거에 기반한 치료 지침 마련이 향후 과제입니다.
8. 참고문헌
섹션 제목: “8. 참고문헌”- Mohan S, Kandle K, Ganesan S, Prakash VJ, Mistry S, Anand AR, et al. Endogenous fungal endophthalmitis following COVID-19 infection with microbiological and molecular biological correlation - A report of two cases. Indian journal of ophthalmology. 2023;71(5):2272-2275. doi:10.4103/ijo.IJO_2044_22. PMID:37202969; PMCID:PMC10391411.
- Awh CC, Mammo DA, Bergstrom R, Baynes K, Srivastava SK. Fungal Endophthalmitis Secondary to Aspergillus terreus Exacerbated by Intravitreal Dexamethasone in a Patient With Sarcoidosis. Journal of vitreoretinal diseases. 2023;7(5):448-454. doi:10.1177/24741264231173207. PMID:37706086; PMCID:PMC10496802.
- Koide R, Yamamoto S, Kobayashi Y, Irie J, Enaida H. ATYPICAL ENDOGENOUS FUNGAL ENDOPHTHALMITIS CAUSED BY CANDIDA RUGOSA. Retinal cases & brief reports. 2023;17(6):672-675. doi:10.1097/ICB.0000000000001275. PMID:35333842; PMCID:PMC10597450.
- Narnaware SH, Bawankule PK, Sontakke S. Misdiagnosed case of fungal endophthalmitis. Eye. 2024;38(1):76-77.
- Huang D, Tran L, Li JY, Lee W, Kim E, Moussa K. Povidone iodine-infused pars plana vitrectomy for severe Arthrographis kalrae fungal endophthalmitis. American journal of ophthalmology case reports. 2024;36:102207. doi:10.1016/j.ajoc.2024.102207. PMID:39553913; PMCID:PMC11566710.
- Fan N, Duan X, Liu X, Fan P, Chen N, Sun J. First Documented Successful Treatment of Chronic Postoperative Fungal Endophthalmitis Induced by Trichosporon Inkin with Fluconazole. Infection and drug resistance. 2024;17:5803-5813. doi:10.2147/IDR.S485152. PMID:39734738; PMCID:PMC11681906.
- Qi C, Mo B, Jiang C, Li J, Bo X, Xiao X, et al. Clinical Characteristics and Treatment Outcomes of Fungal Endophthalmitis Caused by Neoscytalidium dimidiatum. Infection and drug resistance. 2025;18:3671-3675. doi:10.2147/IDR.S517505. PMID:40718366; PMCID:PMC12297007.
- Sugantheran J, Zunaina E, Md Kasim WM, Talib N. Invasive Klebsiella syndrome with coexisting fungal endophthalmitis. Malaysian family physician : the official journal of the Academy of Family Physicians of Malaysia. 2021;16(2):94-97. doi:10.51866/cr1100. PMID:34386173; PMCID:PMC8346748.
- Kaderli ST, Karalezli A, Çitil BE, Saatci AO.. Endogenous Fungal Endophthalmitis in a Patient Admitted to Intensive Care and Treated with Systemic Steroid for COVID-19. Turk J Ophthalmol. 2022;52(2):139-141. doi:10.4274/tjo.galenos.2022.04324. PMID:35481735; PMCID:PMC9069083.
- Durand ML. Bacterial and Fungal Endophthalmitis. Clin Microbiol Rev. 2017;30(3):597-613. doi:10.1128/cmr.00113-16.
- Haseeb AA, Elhusseiny AM, Siddiqui MZ, Ahmad KT, Sallam AB. Fungal Endophthalmitis: A Comprehensive Review. Journal of fungi (Basel, Switzerland). 2021;7(11). doi:10.3390/jof7110996. PMID:34829283; PMCID:PMC8623405.