Netarsudil and ripasudil are Rho-associated kinase (ROCK) inhibitors used as intraocular pressure-lowering agents for open-angle glaucoma and ocular hypertension. Netarsudil is primarily used in the United States, while ripasudil is used in Japan, South Korea, and India.
Common side effects of ROCK inhibitors include conjunctival hyperemia, subconjunctival hemorrhage, cornea verticillata, and pain at the instillation site 1). In addition, a rarer side effect of honeycomb-pattern corneal epithelial edema has been reported 1). This condition is also called reticular bullous epithelial edema or honeycomb corneal edema.
ROCK inhibitors lower intraocular pressure through three mechanisms: promoting aqueous humor outflow from the trabecular meshwork, suppressing aqueous humor production, and reducing episcleral venous pressure. However, the mechanism by which they cause honeycomb-like corneal epithelial edema remains unknown.
QWhat types of ROCK inhibitors are available?
A
The ROCK inhibitors used in ophthalmology are mainly two types: netarsudil (approved in the United States) and ripasudil (approved in Japan). Both are used as eye drops for open-angle glaucoma and ocular hypertension.
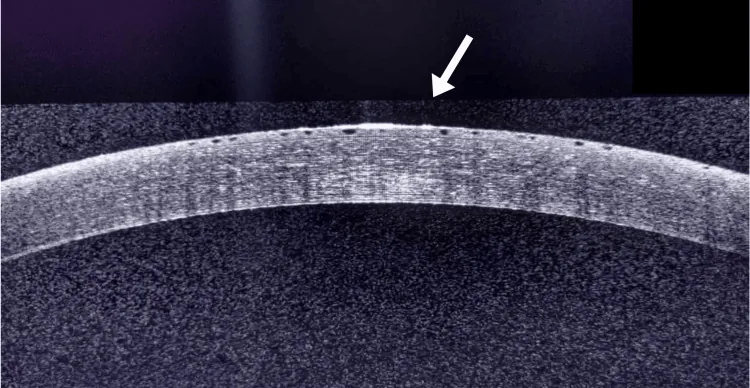
Kamdar GA, Chodvadiya SA, Paranjpe R. Drop and Swell: Unanticipated Corneal Edema From Netarsudil Therapy. Cureus. 2024 Nov 10; 16(11):e73376. Figure 2. PMCID: PMC11631165. License: CC BY.
Anterior segment OCT shows epithelial edema localized to the superficial side, indicated by arrows. This is an appropriate auxiliary image to explain that ROCK inhibitor-related corneal edema is predominantly epithelial.
The main subjective symptoms of ROCK inhibitor-related corneal epithelial edema are shown below.
Blurred vision: Caused by decreased corneal transparency due to corneal epithelial edema. It may lead to severe visual impairment.
Eye pain and irritation: Occurs due to damage to the corneal surface caused by blister formation and epithelial irregularity.
Redness: Accompanied by conjunctival injection. It may overlap with redness caused by the side effects of the ROCK inhibitor itself.
Tearing: Reflex tearing occurs in response to ocular surface irritation.
Symptoms may appear as early as 5 days after starting the medication. In corneal edema, mild cases tend to have worse vision in the morning that improves during the day.
Clinical Findings (Findings Confirmed by Physician Examination)
Characteristic findings observed on slit-lamp microscopy are shown.
Corneal Epithelial Findings
Reticular bullae: Multilobular honeycomb-pattern blisters form in the corneal epithelium. This is a characteristic finding of this disease.
Microcystic edema: Small cyst-like structures are scattered within the epithelium.
Epithelial irregularity: Blisters cause unevenness of the corneal surface.
Anterior Segment OCT Findings
Blisters/honeycomb structure: Blister formation and honeycomb structure in the corneal epithelium can be confirmed on anterior segment OCT.
Epithelial thickening: The thickness of the corneal epithelium increases due to edema.
QWhat does honeycomb-like edema look like?
A
When observed with a slit lamp microscope, a multilobular blister pattern resembling a honeycomb is seen in the corneal epithelium. Anterior segment OCT can also confirm the blister structure, but it is not essential for diagnosis.
The exact mechanism of ROCK inhibitor-associated corneal epithelial edema is unknown. The following risk factors have been reported.
Pre-existing corneal edema: In eyes with reduced corneal endothelial function, the effect of ROCK inhibitors may be amplified.
History of uveitis: Intraocular inflammation may disrupt the blood-aqueous barrier and enhance the drug’s effect on the cornea.
Previous ocular surgery: In eyes after cataract surgery, etc., corneal endothelial cells are reduced, which may make epithelial edema more likely to occur.
However, cases of epithelial edema after starting netarsudil have been reported even in patients without a history of corneal disease or intraocular inflammation. It should be noted that it can occur even without risk factors.
QCan ripasudil cause similar side effects?
A
Most reports are for netarsudil, but since ripasudil also has the same ROCK inhibitory action, similar corneal epithelial edema may occur. Transient morphological changes in corneal endothelial cells have also been observed with ripasudil2).
Diagnosis is made by confirming the following three points.
Medication history: Confirm the start of netarsudil or ripasudil eye drops. Onset typically occurs within days to weeks after initiation.
Slit-lamp examination: Observe characteristic honeycomb-patterned blisters on the corneal epithelium. Also assess the degree of conjunctival injection.
Anterior segment OCT: Useful for confirming the presence of epithelial edema, but not essential for diagnosis. It can visualize intraepithelial blister formation and honeycomb structures.
It is important to differentiate from other diseases that cause corneal epithelial edema.
Differential Diagnosis
Key Differentiating Features
Fuchs endothelial corneal dystrophy
Presence of corneal guttae
Postoperative corneal edema
Temporal relationship with surgery
Herpetic corneal endotheliitis
Keratatic precipitates and anterior chamber inflammation
A history of ROCK inhibitor use and the presence of a honeycomb pattern are most important for differentiating from other corneal edemas 1). In addition to medication history, family history, trauma history, and contact lens wear history should also be confirmed during history taking 1).
The mainstay of treatment is discontinuation of the ROCK inhibitor. In most cases, complete recovery occurs after drug discontinuation. Consult with the primary physician about switching to other glaucoma medications.
In addition to drug discontinuation, the following adjunctive therapies may be used to promote recovery.
Steroid eye drops: Suppress inflammation of the corneal epithelium and promote reduction of edema.
Hypertonic saline eye drops (5% NaCl): Use the osmotic gradient of the corneal epithelium to expel water from the cornea. Corneal dehydration with hypertonic saline is effective in reducing epithelial edema, but does not directly reduce stromal edema.
Antibiotic eye drops: May be used to prevent secondary infection when bullae rupture 1).
If intraocular pressure is near the upper normal limit or elevated, lowering intraocular pressure is also considered useful for improving corneal edema, but choose an antihypertensive drug other than a ROCK inhibitor1). In patients where inflammation may be involved, the use of prostaglandin-related drugs should be avoided 1).
QHow long does it take to recover after stopping the drug?
A
In case reports, improvement of epithelial edema has been observed within 5 weeks after drug discontinuation. Clinically, improvement is confirmed as bullae become smaller and the spaces between bullae widen.
Rho-associated coiled-coil containing protein kinase (ROCK) is a serine/threonine kinase consisting of two isoforms, ROCK1 and ROCK22). It functions as a downstream effector of the small GTPase Rho and is involved in the following cellular functions2):
Cytoskeletal organization: Regulates the reorganization of actin filaments.
Cell migration: Involved in the migration of corneal endothelial cells (CECs) and epithelial cells.
Cell-cell adhesion: Regulates the formation of tight junctions and adherens junctions.
Cell proliferation and apoptosis: Involved in cell cycle control and programmed cell death.
The following possibilities have been considered as mechanisms by which ROCK inhibitors cause edema in the corneal epithelium:
Impaired epithelial barrier function: Relaxation of tight junctions due to ROCK inhibition may reduce the barrier function of the epithelium, increasing water influx from the tear side into the epithelium.
Effects on the cytoskeleton: Reorganization of the actin cytoskeleton due to ROCK inhibition may alter the morphology and function of epithelial cells.
Indirect effects on the corneal endothelium: It has been reported that ripasudil eye drops cause transient morphological changes (e.g., unclear cell borders) in corneal endothelial cells even in healthy individuals2). This may lead to epithelial edema through effects on endothelial pump function.
The reason for the characteristic honeycomb pattern is unknown, but water accumulation along the tight junction structures between corneal epithelial cells may be involved.
7. Latest Research and Future Perspectives (Research-stage Reports)
ROCK inhibitors are drugs that have been attempted for the treatment of corneal diseases. They have been confirmed to promote adhesion, proliferation, and migration of corneal endothelial cells, and their potential as therapeutic agents for Fuchs endothelial corneal dystrophy and bullous keratopathy is being studied2).
A report indicates that combined therapy with cultured corneal endothelial cells and ROCK inhibitors via intracameral injection achieved corneal thickness less than 630 μm in 10 out of 11 bullous keratopathy patients, and visual improvement was obtained in 9 cases2).
Thus, ROCK inhibitors have both a therapeutic aspect of promoting corneal endothelial regeneration and a side effect aspect of corneal epithelial edema. Future research will focus on elucidating the mechanism of epithelial edema and identifying risk factors.
Elucidation of the precise mechanism of honeycomb-like epithelial edema
Search for biomarkers to predict the risk of onset
Relationship between isoform selectivity of ROCK inhibitors and side effect profile
Establishment of optimal administration method for corneal endothelial therapeutic application of ROCK inhibitors
QAre ROCK inhibitors good or bad for the cornea?
A
ROCK inhibitors have a therapeutic effect of promoting proliferation and migration of corneal endothelial cells, but on the other hand, side effects of causing corneal epithelial edema have been reported in rare cases. For details, refer to the section “Pathophysiology / Detailed Mechanism of Onset”. Elucidation of the mechanism of this dual nature is a future research topic.