Rhinosporidiosis is a rare chronic granulomatous infection caused by the endospore-forming microorganism Rhinosporidium seeberi. It was first reported in 1900 by Guillermo Seeber in Buenos Aires as a vascular nasal polyp. In 1923, Ashworth described its life cycle and established the scientific name.
Its classification was debated for many years, but phylogenetic analysis of ribosomal DNA revealed that it belongs to Mesomycetozoea, a group positioned at the boundary between fungi and fish parasites 3). It cannot be cultured on artificial media, and drug susceptibility testing has not yet been established.
Over 90% of cases are reported from the Indian subcontinent, and it is endemic in India, Sri Lanka, Pakistan, Africa, and South America 4). The nasopharynx is the most commonly affected site (over 70%), and ocular involvement accounts for about 15%. In the eye, the conjunctiva accounts for 69% and the lacrimal sac for 24% 2). A literature review of lacrimal sac rhinosporidiosis reported 156 cases 1).
Human-to-human transmission has not been confirmed, and it is not considered a contagious disease. Cases have also been reported in animals such as dogs, cats, horses, and cattle.
QCan rhinosporidiosis be transmitted from person to person?
A
Human-to-human transmission has not been confirmed. Infection with R. seeberi occurs through damaged epithelium after contact with contaminated stagnant water or soil. Therefore, it is not a contagious disease, and patient isolation is unnecessary.
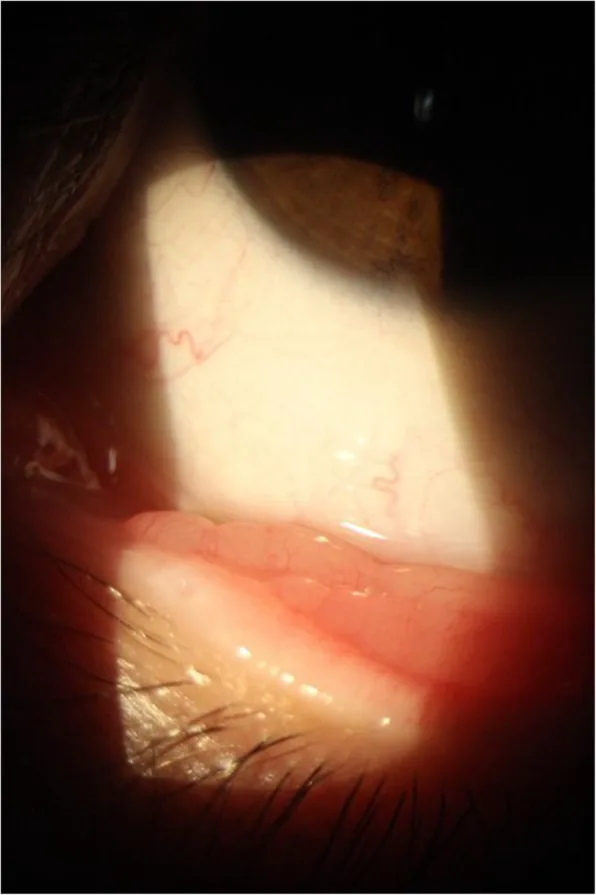
Almeida FA, Teixeira-Junior AAL, Pinho JD, et al. Evaluation of diagnosed cases of eye rhinosporidiosis in a public hospital of Maranhão, Northeast Brazil. BMC Ophthalmology. 2019 Nov 8; 19:218. Figure 4. PMCID: PMC6842159. License: CC BY.
A slit-lamp image shows a whitish elevated lesion on the conjunctiva. The superficial vascular pattern and the spread of the polypoid lesion are visible, making it easy to understand the appearance as a conjunctival lesion.
Conjunctival lesion: A granular, fleshy, red soft tissue lesion. Numerous pinhead-sized white to yellow spots are seen on the surface, reflecting mature sporangia. It is highly vascular and fragile, bleeding easily on contact.
Morphology of conjunctival lesion: On the palpebral conjunctiva, it is pedunculated; on the bulbar conjunctiva, it becomes flat and sessile due to eyelid pressure.
Lacrimal sac lesion: Presents as a soft swelling from the inner canthus to the lower eyelid. Obstruction is confirmed by lacrimal sac irrigation. CT shows a solid mass in the lacrimal sac area1)2)
Disseminated lesions: Rarely, multiple subcutaneous nodules appear on the extremities and trunk. May be accompanied by osteolytic bone lesions or pulmonary lesions3)4)
QHow is lacrimal sac rhinosporidiosis differentiated from chronic dacryocystitis?
A
Lacrimal sac rhinosporidiosis is clinically similar to chronic dacryocystitis and is often misdiagnosed1). CT is useful for differentiation, evaluating the presence of a solid mass within the lacrimal sac and bone erosion2). In endemic areas, lacrimal sac swelling, especially with bloody tears, should raise suspicion. Definitive diagnosis is made by histopathological examination.
R. seeberi exists in stagnant water and soil, infecting mucosa through damaged epithelium. The highest incidence is reported among river sand collectors6). Infection occurs when endospores are inoculated into damaged epithelium.
Infection of the lacrimal sac is thought to spread ascendingly from nasal lesions via the nasolacrimal duct2). However, some researchers deny transmission via the nasolacrimal duct due to the presence of valves1). Routes via the conjunctiva through the lacrimal canaliculi, or via subconjunctival connective tissue and lymphatics, have also been reported1).
Definitive diagnosis is based on histopathological examination. Tissue is obtained by excisional biopsy, scraping of surface lesions, or fine-needle aspiration.
Histological findings include multiple sporangia at various stages of maturity, surrounded by a thin wall. Sporangia are 50–1000 μm in diameter and contain endospores approximately 5–10 μm in size. Surrounding tissue shows hyperplasia and loose fibrovascular stroma with infiltration of lymphocytes, macrophages, plasma cells, and polymorphonuclear leukocytes.
An important feature is the near absence of eosinophils at the infection site and the lack of a Splendore-Hoeppli reaction.
For lacrimal sac lesions, contrast-enhanced CT is performed to evaluate the extent of the mass and the presence of bone erosion 1)2). If extension to the nasolacrimal duct is suspected, CT dacryocystography (CT-DCG) is recommended 2).
QHow do you differentiate Coccidioides from rhinosporidiosis?
A
Both are histologically similar, appearing as large, thick-walled spherules containing endospores. Mucicarmine staining is useful for differentiation: R. seeberi is positive, while Coccidioides immitis is negative. Additionally, the endospores of R. seeberi are larger and more numerous than those of C. immitis.
The first choice is surgical excision plus electrocautery. Electrocautery is useful for minimizing bleeding and preventing the spread of endospores to the surrounding mucosa. Complete excision is important because spillage of endospores can cause recurrence 5)6).
Treatment of Conjunctival Lesions
Complete excision + electrocautery: After complete excision of the polyp, the base is cauterized. To prevent the spread of endospores, care must be taken to avoid contamination of surrounding tissues during excision.
Postoperative management: Regular follow-up is necessary to monitor for recurrence. The recurrence rate of ocular rhinosporidiosis is lower than that of nasopharyngeal lesions.
Treatment of Lacrimal Sac Lesions
Dacryocystectomy: Complete removal of the entire lacrimal sac is recommended 1). Postoperative dapsone therapy is usually recommended 2).
Endoscopic dacryocystorhinostomy (endoscopic DCR): The mass within the lacrimal sac is excised and the lacrimal drainage pathway is reconstructed 1)2). This avoids an external incision and reduces the risk of dissemination to scar tissue.
Grading of lacrimal sac involvement: Treatment is selected based on classification into Grade 1 (lacrimal sac and nasolacrimal duct only), Grade 2 (combined nasal and ocular involvement), and Grade 3 (lacrimal sac-cutaneous fistula) 2).
Dapsone is used as an adjunct to surgical treatment. It is administered at 100 mg/day for 3 to 6 months 2). It is thought to inhibit sporangial maturation and promote stromal fibrosis.
In disseminated disease where dapsone cannot be used, a combination therapy of liposomal amphotericin B + ketoconazole + cycloserine has been reported to be effective 3).
The prognosis is generally good. Localized lesions can be cured by complete excision. However, recurrence rates vary by site: approximately 10% for nasal lesions and approximately 40% for lacrimal sac lesions 2). Disseminated infection is rare, but if bone destruction or brain involvement occurs, it can be fatal.
QWhat are the side effects of dapsone?
A
The main side effect of dapsone is hemolytic anemia, which can be severe especially in patients with G6PD deficiency. Quantitative testing of G6PD activity is necessary before administration. Rarely, dapsone-induced autoimmune hemolytic anemia (positive direct antiglobulin test) has been reported 3). Methemoglobinemia also requires attention as a complication during general anesthesia 2).
When endospores of R. seeberi are inoculated into tissue through damaged epithelium, they develop into young sporangia called trophocytes. Trophocytes are 10–100 μm in size and have a single-layered cell wall. As they grow, they become intermediate sporangia, forming a larger, thicker double-layered wall.
Mature sporangia reach about 100–300 μm, are filled with numerous endospores, and are surrounded by immune cells. Upon stimulation by moisture, the sporangium ruptures, releasing endospores, and the infection and life cycle continue.
Rapid replication occurs in the mucosa at the infection site, leading to hyperplasia of host tissue and recruitment of local immune responses. Granulomas form and develop into multilobed, vascular, polypoid masses. Rupture of sporangia can trigger a giant cell reaction.
R. seeberi possesses multiple immune evasion mechanisms, including immune deviation, local immunosuppression, immunoglobulin binding, and antigenic variation 5). A shift from Th-1 to Th-2 immune response is also thought to contribute to persistent infection 6).
Although usually confined to local lesions, hematogenous or lymphatic dissemination can occur 3). Inadvertent spillage of endospores during surgery can cause secondary implantation at distant sites 5). Dissemination to the bronchus after nasal surgery has been explained by this mechanism 5).
QWhy does rhinosporidiosis tend to recur?
A
The main cause of recurrence is spillage of endospores during surgery. Incomplete resection or inadequate electrocautery can scatter endospores into the surrounding mucosa. Additionally, R. seeberi has multiple immune evasion mechanisms that suppress the host immune response, making infection control difficult 5). To prevent recurrence, complete resection, sufficient cauterization of the base, and postoperative dapsone administration are important.
For cases of disseminated rhinosporidiosis where dapsone cannot be used, a report indicates that combination therapy with liposomal amphotericin B + ketoconazole + cycloserine was effective 3). Each drug has anti-spore activity against R. seeberi, and after 5 months of treatment, many lesions shrank or disappeared 3).
For lacrimal sac rhinosporidiosis, a three-stage grading system has been proposed and is used to select the optimal surgical procedure based on the extent of the lesion 2). Advances in endoscopic techniques have enabled minimally invasive surgery that avoids external incisions, and a reduction in recurrence rates is expected 1).
Reports of sporadic cases from non-endemic regions (such as Malaysia and Japan) are increasing 4)6), and there is a need for improved global awareness of the disease. The difficulty in culturing R. seeberi remains a barrier to drug development and is a future research challenge.
Pradhan P, Samal S. Rhinosporidiosis of the lacrimal sac masquerading as chronic dacryocystitis: a rare presentation. Autopsy & case reports. 2021;11:e2020214. doi:10.4322/acr.2020.214. PMID:33968816; PMCID:PMC8020589.
Parida PK, Thangavel S, Raja K, Saxena SK. Lacrimal sac rhinosporidiosis. BMJ case reports. 2021;14(6). doi:10.1136/bcr-2021-243926. PMID:34183318; PMCID:PMC8240581.
Ghosh R, Mondal S, Roy D, Ray A, Mandal A, Benito-León J. A case of primary disseminated rhinosporidiosis and dapsone-induced autoimmune hemolytic anemia: A therapeutic misadventure. IDCases. 2021;24:e01076. doi:10.1016/j.idcr.2021.e01076. PMID:33816117; PMCID:PMC8010393.
Ahmad MF, Samri SB, Ahmed WAW, Jalil NAC, Sapiai NA. A rare case of disseminated rhinosporidiosis mimicking tuberculosis. IDCases. 2024;36:e02009. doi:10.1016/j.idcr.2024.e02009. PMID:38947561; PMCID:PMC11214292.
Nagi K, Sekar R, Saxena SK, Stephen N. Naso-Bronchial Rhinosporidiosis. BMJ case reports. 2022;15(2). doi:10.1136/bcr-2021-247133. PMID:35140090; PMCID:PMC8830203.
Bano G, Angral S, Sasanka KSBS, Varshney S, Sarangi PK. A Rare Case of Nasal Rhinosporidiosis in the Santhal Pargana Region of Jharkhand: Clinical Presentation and Management. Cureus. 2024;16(10):e72674. doi:10.7759/cureus.72674. PMID:39618667; PMCID:PMC11605488.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.