
Ocular Neuropathic Pain (Corneal Neuropathic Pain)
Key points at a glance
Section titled “Key points at a glance”1. What is Ocular Neuropathic Pain?
Section titled “1. What is Ocular Neuropathic Pain?”Ocular neuropathic pain (corneal neuropathic pain: CNP) is persistent chronic pain despite minimal organic findings in the cornea or ocular surface 1). It is also called “pain without stain” or “phantom cornea.” It generally refers to a condition where abnormal pain responses occur to non-noxious stimuli 1).
Sensory nerves of the cornea and conjunctiva form the afferent pathway of the lacrimal functional unit and are involved in the tear secretion reflex 4).
Corneal sensory nerve fibers are functionally classified into three types 4):
- Polymodal nociceptors: Constitute about 70% of all fibers. Respond to mechanical, chemical, and thermal stimuli; about 60% contain CGRP (calcitonin gene-related peptide)
- Mechanoreceptors: About 20%. Respond specifically to physical stimuli
- Cold receptors: 10–15%. Respond to temperature changes
CNP is broadly classified into peripheral and central types based on pathogenesis 1). Peripheral CNP results from direct damage to corneal nerves, while central CNP is due to neuroplastic changes at the brainstem or thalamic level. Mixed cases are common.
Dry eye is primarily characterized by tear film instability and ocular surface inflammation, with objective findings on fluorescein staining or Schirmer test. In contrast, ocular neuropathic pain is a condition in which severe pain persists despite the absence of notable organic corneal findings. However, both conditions can coexist, so differentiation is made using the proparacaine test described in the Diagnosis and Examination Methods section.
2. Main Symptoms and Clinical Findings
Section titled “2. Main Symptoms and Clinical Findings”Subjective Symptoms
Section titled “Subjective Symptoms”The subjective symptoms of CNP are diverse and qualitatively different from those of typical dry eye 1).
- Burning sensation and stinging: The most frequent complaint. Persistent and difficult to relieve with standard eye drops.
- Photoallodynia: Eye pain triggered by light stimuli that would not normally cause pain 1).
- Foreign body sensation and dryness: May be reported even when tear volume is normal.
- Facial dystonia and blepharospasm: Reflex muscle tension associated with pain.
- Psychiatric comorbidities: Anxiety disorders, depression, and migraine are frequently associated 1).
Symptoms show diurnal variation and are often exacerbated by environmental factors such as wind, air conditioning, and screen viewing.
Clinical Findings
Section titled “Clinical Findings”Slit-lamp examination characteristically reveals no significant corneal epithelial damage (“pain without stain”). Mild tear film instability may be present, but it is disproportionate to the severity of subjective symptoms 1).
In vivo confocal microscopy (IVCM) detects the following findings 1)2):
- Neuroma: Abnormal enlargement of damaged corneal nerves.
- Decreased corneal nerve density: reduction of the sub-basal nerve plexus
- Increased dendritic cells: reflects chronic neurogenic inflammation
- Tortuosity and beading of nerve fibers: signs of nerve degeneration3)
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”The causes of CNP are broadly divided into direct damage to peripheral nerves and secondary neuropathy due to chronic inflammation.
- Refractive surgery: LASIK, PRK, etc., where corneal nerves are cut during flap creation, can trigger chronic pain1). SMILE also cannot completely avoid nerve damage.
- Dry eye: Persistent chronic ocular surface inflammation leads to sensitization of corneal nerves1)
- Herpes virus infection: Damages corneal sensory nerves and may transition to neuropathic pain after infection
- Diabetes: Affects corneal nerves as part of metabolic peripheral neuropathy
- Sjögren’s syndrome: Prone to neuropathic hypersensitivity4)
- Drug-induced corneal disorders: Neurotoxicity from long-term use of eye drops containing BAC (benzalkonium chloride)
Differentiation from trigeminal neuralgia is also important. Trigeminal neuralgia has an incidence of 4–5 per 100,000 people and is more common in elderly women. It differs from CNP in that carbamazepine is effective.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”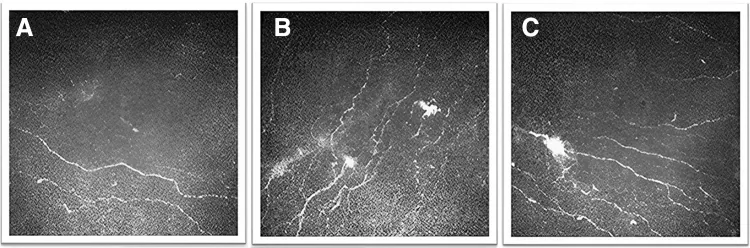
The diagnosis of CNP begins with recognizing “pain disproportionate to organic findings” 1). First, slit-lamp microscopy and tear film tests are performed to rule out other ocular surface diseases, and then the following tests are conducted.
Proparacaine Challenge Test
Section titled “Proparacaine Challenge Test”The change in pain after instillation of 0.5% proparacaine helps differentiate between peripheral and central causes 1).
| Pain Change | Judgment | Meaning |
|---|---|---|
| Complete resolution | Peripheral | Corneal nerve abnormality is the main cause |
| No change | Central | Brainstem/thalamic sensitization is the main cause |
| Partial reduction | Mixed | Both mechanisms are involved |
In Vivo Confocal Microscopy (IVCM)
Section titled “In Vivo Confocal Microscopy (IVCM)”It is the only non-invasive test that can observe the corneal nerve plexus at the cellular level 1)2). It detects findings such as neuromas, decreased nerve density, increased dendritic cells, and beading 3). Its use as an objective diagnostic marker is advancing.
Pain Assessment Questionnaires
Section titled “Pain Assessment Questionnaires”- OPAS (Ocular Pain Assessment Survey): Quantifies the intensity, frequency, and impact on daily life of eye pain 1)2)
- NPSI-Eye (Neuropathic Pain Symptom Inventory for the Eye): A questionnaire specific to neuropathic pain 1)
Differentiation from neurotrophic keratopathy is also necessary. The Mackie classification categorizes it into stage 1 (punctate superficial keratopathy), stage 2 (persistent epithelial defect), and stage 3 (corneal ulcer/perforation). Neurotrophic keratopathy is characterized by “no pain,” whereas CNP is characterized by “pain without findings,” representing contrasting conditions.
It is a simple test in which 0.5% proparacaine (a local anesthetic) is instilled and the change in pain is evaluated. In peripheral cases, pain disappears after instillation, while in central cases, pain persists. Since treatment strategies differ based on the results, it provides important information for selecting stepwise treatment as described in Standard Treatment.
5. Standard Treatment
Section titled “5. Standard Treatment”A stepwise approach (treatment ladder) is recommended for the treatment of CNP 1). First, start with topical treatment, and if insufficient, proceed to systemic medications, adjunctive therapies, and surgical interventions. Multidisciplinary collaboration including psychiatry is important 1).
Topical Treatment (Step 1)
Section titled “Topical Treatment (Step 1)”- Corticosteroid eye drops: Suppress neurogenic inflammation and reduce dendritic cell density 2). Use only for a short period.
- Autologous serum eye drops (20%): Contain neurotrophic factors (e.g., NGF) and promote nerve regeneration 3). A report showed improvement in pain scores from 9.1 to 3.1 with a median treatment duration of 3.8 months 3)
- Lacosamide 1% eye drops: A sodium channel blocker that suppresses the excitation of cold-sensitive nerves 2). An in-hospital preparation made from Vimpat 10 mg/mL, stable for 14 days under refrigeration 2)
- Low-dose naltrexone (LDN) 0.001–0.2% eye drops: Exerts anti-inflammatory and analgesic effects through opioid antagonism via Toll-like receptors (TLR) 2)
Systemic Medications (Second Step)
Section titled “Systemic Medications (Second Step)”If local treatment is insufficient, systemic medications are added, especially for central CNP 1).
| Drug | Dosage | Drug Class |
|---|---|---|
| Gabapentin | 100–900 mg 3 times/day | Antiepileptic |
| Pregabalin | 25–200 mg 2 times/day | Antiepileptic |
| Nortriptyline | 10–100 mg/day | Tricyclic Antidepressant |
| Duloxetine | 20–60 mg/day | SNRI |
Carbamazepine 100–400 mg twice daily is effective for trigeminal neuralgia and is also used for CNP1). In Japan, it is widely used as a first-line treatment for trigeminal neuralgia.
Adjunctive Therapy (Stage 3)
Section titled “Adjunctive Therapy (Stage 3)”- Botulinum toxin injection: Useful in cases with blepharospasm or facial dystonia1)
- Transcutaneous electrical nerve stimulation (TENS): Reported as a non-invasive pain relief method for ocular pain7)
- Nerve block: Such as supraorbital nerve and supratrochlear nerve blocks1)
Surgical Treatment (Stage 4)
Section titled “Surgical Treatment (Stage 4)”- Amniotic membrane transplantation (AMT): Suppresses ocular surface inflammation and provides neuroprotection1)
- Corneal neurotization: Includes direct method (transplantation of the contralateral supraorbital nerve) and indirect method (using autologous nerve grafts such as the sural nerve)6). Sensory recovery takes 6–12 months6)
Autologous serum eye drops are a special type of eye drops prepared from the patient’s own blood, and may be difficult to obtain at general clinics. It is advisable to consult a university hospital or a corneal specialty center. For details, refer to the Topical Therapy section.
The duration varies greatly among individuals. In cases that improve with topical therapy alone, it may take several months; in cases requiring systemic medications, treatment may be needed for years. It is important to adjust treatment stepwise and monitor progress.
6. Pathophysiology and Detailed Mechanisms
Section titled “6. Pathophysiology and Detailed Mechanisms”The pathophysiology of CNP involves two mechanisms, peripheral sensitization and central sensitization, which interact in a layered manner 1).
Peripheral Sensitization
Section titled “Peripheral Sensitization”Damage to corneal nerves (due to surgery, infection, inflammation, etc.) leads to the formation of neuromas 1)2). At the site of injury, the following ion channels are upregulated:
- Nav1.7: Voltage-gated sodium channel. Lowers the threshold for ectopic firing.
- TRPV1: Vanilloid receptor involved in nociception. Increases sensitivity to thermal and chemical stimuli.
- TRPM8: Channel expressed in cold receptors. Minor temperature changes due to tear evaporation can trigger pain 2).
These changes cause ectopic firing even with weak stimuli that normally do not cause pain, leading to allodynia.
Neurogenic Inflammation
Section titled “Neurogenic Inflammation”Damaged sensory nerve endings release CGRP and substance P (SP) 4). CGRP causes vasodilation, and SP increases vascular permeability, triggering local neurogenic inflammation 4). After nerve transection, denervation hypersensitivity in lacrimal gland secretion has been reported 4).
Central Sensitization
Section titled “Central Sensitization”Persistent nociceptive input from the periphery induces plastic changes in neurons of the brainstem trigeminal nucleus and thalamus 1). Upregulation of NMDA receptors is a key molecular mechanism, leading to long-term enhancement of synaptic transmission efficiency. At this stage, pain becomes difficult to improve with peripheral nerve treatment alone.
Mechanism of Action of Autologous Serum Eye Drops
Section titled “Mechanism of Action of Autologous Serum Eye Drops”Anam et al. (2024) reported the multifaceted mechanism of action of autologous serum eye drops 3). In addition to promoting nerve regeneration via NGF (nerve growth factor), microRNA-mediated gene expression regulation within exosomes, modulation of TRPV1 receptor activity, and reduction of substance P levels collectively contribute to nerve repair. After 3.8 months of treatment with 20% autologous serum eye drops, the photophobia score improved from 8.8 to 1.6, and IVCM showed increased nerve fiber density and length, along with decreased neuromas and beading 3).
7. Latest Research and Future Perspectives (Research-stage Reports)
Section titled “7. Latest Research and Future Perspectives (Research-stage Reports)”Nerve Growth Factor (NGF) Preparations
Section titled “Nerve Growth Factor (NGF) Preparations”rhNGF (cenegermin) showed efficacy for neurotrophic keratopathy in the REPARO trial (Phase I/II) 5). Topical application promotes corneal nerve regeneration and epithelial healing. Application to CNP is still at the research stage, but combination with DHA (docosahexaenoic acid) has been reported to further promote nerve regeneration 5).
Standardization of Blood-Derived Eye Drops
Section titled “Standardization of Blood-Derived Eye Drops”In addition to autologous serum eye drops, various blood-derived preparations such as cord blood platelet lysate and panretinal photocoagulation (platelet-rich plasma) are being developed 3). However, standardization of preparation protocols and concentrations remains a challenge, and large-scale long-term comparative trials are needed 3).
IVCM as a Diagnostic Marker
Section titled “IVCM as a Diagnostic Marker”Efforts are underway to establish findings detected by IVCM, such as neuroma, decreased nerve density, and increased dendritic cells, as objective diagnostic markers 1)2). Advances in image analysis technology are expected to improve the accuracy of quantitative assessment.
Enkephalin Modulators
Section titled “Enkephalin Modulators”A new approach that inhibits the degradation of endogenous enkephalins (endogenous opioids) to enhance local analgesic effects is being studied 2). By enhancing endogenous pain relief mechanisms rather than directly stimulating opioid receptors, the risk of dependence is considered low.
Intranasal Nerve Stimulation
Section titled “Intranasal Nerve Stimulation”A method involving insertion of an electrical stimulation device into the nasal cavity to stimulate the trigeminal nerve and induce tear secretion and analgesic effects is being investigated 1). As a non-invasive treatment option, future clinical trial results are anticipated.
8. References
Section titled “8. References”- Watson SL, Le DTM. Corneal neuropathic pain: a clinical practice narrative review. Eye. 2024;38:2350-2358.
- Nortey J, Smith D, Seitzman GD, Gonzales JA. Topical Therapeutic Options in Corneal Neuropathic Pain. Frontiers in pharmacology. 2021;12:769909. doi:10.3389/fphar.2021.769909. PMID:35173607; PMCID:PMC8841414.
- Anam A, Liu C, Tong L, Liu YC. Blood-Derived Eye Drops for the Treatment of Corneal Neuropathic Pain. Journal of ocular pharmacology and therapeutics : the official journal of the Association for Ocular Pharmacology and Therapeutics. 2024;40(5):281-292. doi:10.1089/jop.2023.0155. PMID:38648544; PMCID:PMC11296151.
- Dartt DA. Neural regulation of lacrimal gland secretory processes: relevance in dry eye diseases. Prog Retin Eye Res. 2009;28(3):155-177. doi:10.1016/j.preteyeres.2009.04.003.
- Levi N Kanu, Joseph B Ciolino. Nerve Growth Factor as an Ocular Therapy: Applications, Challenges, and Future Directions. Seminars in Ophthalmology. 2021;36(4):224-231. doi:10.1080/08820538.2021.1890793.
- Dragnea DC, Krolo I, Koppen C, Faris C, Van den Bogerd B, Ní Dhubhghaill S. Corneal neurotization-indications, surgical techniques and outcomes. J Clin Med. 2023;12(6):2214. doi:10.3390/jcm12062214.
- Jones L, Downie LE, Korb D, et al. TFOS DEWS III management and therapy report. Ocul Surf. 2023;22:100901.