Essential blepharospasm refers to repeated, unexplained, intermittent involuntary closure of both eyelids. It is defined as a condition in which the orbicularis oculi and other eyelid-closing muscles contract too strongly, either intermittently or continuously, causing involuntary eyelid closure, with no other neurological or eye disorder as the cause.
In normal blinking, the eyelid-closing muscles (orbicularis oculi, corrugator supercilii, and procerus) and the eyelid-opening muscles (levator palpebrae superioris and frontalis) are inhibited at the same time. In blepharospasm, this simultaneous inhibition is lost, and overcontraction of the eyelid-closing muscles is no longer controlled. It is considered a focal dystonia, with a presumed disorder of the basal ganglia.
Type A botulinum toxin injection (Botox injection) is the first-choice treatment for blepharospasm. After being taken up by the nerve terminal, botulinum toxin acts on synaptic vesicle membrane proteins and inhibits acetylcholine release. This relaxes the target muscle and improves involuntary eyelid closure.
Hemifacial spasm is a different condition from essential blepharospasm. In the posterior cranial fossa, the facial nerve is compressed by blood vessels such as the basilar artery or anterior inferior cerebellar artery, and, rarely, by a tumor or aneurysm, causing spasm through intraneural short-circuiting. A key distinction from essential blepharospasm is that it is unilateral.
QWhat kind of disease is blepharospasm?
A
It is an involuntary movement in which both eyelids close forcefully without the person’s will. It is a focal dystonia in which the simultaneous inhibition between the muscles that close and open the eyelids is lost, and it is more common in women over 60. It is chronic and progressive, rarely goes away on its own, and if it worsens, the person may not be able to open the eyes and may develop functional blindness. It is important to distinguish it from dry eye and orbicularis oculi myokymia.
Essential blepharospasm and Meige syndrome are thought to be part of the same spectrum of focal dystonia, and basal ganglia dysfunction is suspected. In Meige syndrome, involuntary facial movements such as lip dyskinesia occur in addition to blepharospasm.
Factors that worsen it: bright light, fatigue, reading, crowds
Factors that lessen it: darkness, sleep, lying down, pressure on the eyebrow area and similar places (sensory trick)
It is chronic and progressive, and spontaneous recovery is rare. Because spasms and the effort to open the eyelids oppose each other, loosening of the surrounding tissues (drooping eyebrows, ptosis, skin laxity) occurs. As it progresses, inability to open the eyelids leads to functional blindness. In the end, about 15% of patients reach a state of functional blindness.
Blepharospasm is more common in women over 60. It is chronic and progressive, and it rarely resolves on its own. In the long term, spasms eventually stop in about 10% of cases, but about 15% progress to functional blindness. Essential blepharospasm and Meige syndrome are focal dystonias on the same spectrum, and in both, basal ganglia dysfunction is central to the pathophysiology.
The 2011 Blepharospasm Clinical Practice Guideline (Japanese Ophthalmological Society)1) recommends trying to trigger spasms with the blink test. The following three tests are performed in order to assess severity.
Test
Method
Abnormal findings
Rapid blink test
Perform gentle, as fast as possible blinking for 10 to 30 seconds
Only forceful blinking; involuntary movements of other facial muscles
Light blink test
Perform voluntary blinking
The eyebrow area moves; blinking becomes impossible
Forceful blink test
Repeated opening of the eyes after forceful eye closure
Unable to open the eyes; strong facial muscle spasm contraction
As rapid blinking and light blinking become irregular, severity increases as only forceful blinking is possible, and then as opening the eyes becomes difficult or impossible1).
If hemifacial spasm is suspected, an MRI of the brainstem is performed. In the posterior fossa, it is confirmed whether the facial nerve is being compressed by a blood vessel such as the basilar artery or anterior inferior cerebellar artery, or by a tumor or aneurysm, and the cause of the compression is identified.
QHow is blepharospasm diagnosed?
A
Diagnosis is made by trying to trigger the spasm with blink tests (rapid, light, and forceful blinking). Severity is judged by findings such as being able to do only forceful blinking when rapid light blinking is continued, or being unable to open the eyes after forceful eye closure. In hemifacial spasm, MRI is used to confirm vascular compression of the facial nerve.
Botulinum toxin type A injection is indicated for essential blepharospasm, Meige syndrome, and hemifacial spasm. The procedure is performed in consultation with a registered physician who administers botulinum toxin injections.
Botulinum toxin is taken up by the nerve terminals at the neuromuscular junction and acts on synaptic vesicle membrane proteins to block the release of acetylcholine. This relaxes the target muscles and improves involuntary eyelid closure.
Effectiveness: 90%
Onset of effect: latency of 2 to 3 days after injection
Duration of effect: 3 to 4 months (temporary because neuromuscular transmission resumes as nerve collateral sprouts form)
Repeat injection: repeated injections are needed regularly after the effect wears off
In rare cases, neutralizing (blocking) antibodies against botulinum toxin type A are produced. In such cases, type F toxin is effective, but note that its duration is shorter2).
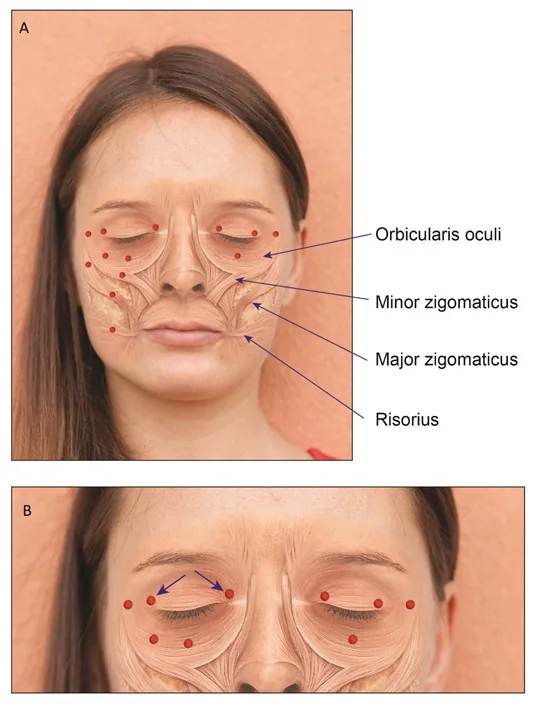
Yahalom G, Janah A, Rajz G, Eichel R. Therapeutic Approach to Botulinum Injections for Hemifacial Spasm, Synkinesis and Blepharospasm. Toxins (Basel). 2022;14(5):362. Figure 3. PMCID: PMC9147094. DOI: 10.3390/toxins14050362. License: CC BY 4.0.
A diagram showing injection points into the orbicularis oculi, corrugator supercilii, and procerus muscles as red dots on a facial anatomy illustration, with arrows indicating the needle insertion direction into the orbital and palpebral parts of the orbicularis oculi. It gives an intuitive view of the distributed injection pattern into both eyelids for blepharospasm and corresponds to the technique of distributed injections into the orbicularis oculi and corrugator supercilii described in the main text section on injection sites and technique.
Injection sites for blepharospasm
Corrugator supercilii muscle: Insert the needle into the head of the eyebrow and inject while touching the bone with the needle tip.
Orbicularis oculi muscle: Because it is a circular muscle, inject it evenly in a distributed pattern. Inject into the muscle near the inner and outer corners of the upper and lower eyelids, on the temple side of the outer corner, and at the outer one-third of the orbital margin of the lower eyelid.
Additional sites for Meige syndrome
In addition to the basic sites, additional injections are given into the zygomaticus major and levator labii superioris alaeque nasi muscles.
Example injection plan: 16 sites in total, 2.5 units each.
QHow long does Botox injection last?
A
The effect appears in 2 to 3 days after injection and lasts for 3 to 4 months. The effectiveness rate is high at 90%. The effect is not permanent, and repeat injections are needed because transmission resumes as collateral nerve branches sprout. Rarely, the effect may be weakened if neutralizing antibodies are produced.
Drug therapy is based on three pharmacologic hypotheses (excess acetylcholine, reduced GABA, and excess dopamine). Lorazepam, clonazepam, and trihexyphenidyl are used, but none are covered by insurance. The response rate is low, around 15%, and because effectiveness varies greatly from person to person, it is best to leave treatment to an experienced neurologist.
Posterior fossa microvascular decompression (neurosurgery) is highly effective as a curative treatment. Botulinum toxin therapy is currently widely used as the first-line treatment.
Sensory stimulation with a headband or tight-fitting glasses
Tinted glasses (for light-triggered cases and cases with photophobia)
Crutch glasses
Rest and artificial tears
Oral combination of anticholinergic, antidopaminergic, and antidepressant drugs
QAre there treatments other than Botox injections?
A
Drug therapy (such as lorazepam and clonazepam) exists, but the response rate is low, at about 15%. Surgical options include orbicularis oculi muscle resection (Anderson method) and partial facial nerve section. As conservative treatment, tinted glasses, crutch glasses, and sensory stimulation with a headband are used as supportive measures. In hemifacial spasm, posterior fossa neurovascular decompression is curative.
Essential blepharospasm and Meige syndrome are focal dystonias, and basal ganglia dysfunction is thought to be involved. Normally, when blinking, the eyelid-closing muscle group (orbicularis oculi, corrugator supercilii, procerus) and the eyelid-opening muscle group (levator palpebrae superioris, frontalis) are inhibited at the same time, but in patients this simultaneous inhibition between the two muscle groups is lost. As a result, overcontraction of the eyelid-closing muscles is not controlled, and involuntary eyelid closure is repeated.
Botulinum toxin type A is taken up by nerve terminals at the neuromuscular junction and acts on synaptic vesicle membrane proteins (such as SNAP-25). This prevents acetylcholine-containing vesicles from fusing with the membrane, blocking the release of acetylcholine. As a result, neuromuscular transmission is blocked and the target muscle relaxes.
About 3 to 4 months after injection, axonal sprouting occurs on the nerve side, forming new neuromuscular pathways. This restores muscle contraction and the effect wears off. This is why regular reinjection is needed. With long-term, high-dose, frequent treatment, neutralizing antibodies may be produced, and if the effect of type A toxin is lost, switching to type F toxin is an option.
In the posterior cranial fossa, the facial nerve is compressed by vessels such as the basilar artery and the anterior inferior cerebellar artery. This persistent stimulation from compression and abnormal discharges within the nerve cause involuntary contraction of the facial muscles. Microvascular decompression surgery, which separates the compressing vessel from the nerve, is effective as a definitive treatment.