Eyelid twitching (orbicularis myokymia) is a relatively slow, worm-like involuntary movement of the orbicularis oculi muscle. It is caused by hyperfunction of the facial nerve and is the most common type of spasmodic eye disorder. It often occurs on the temporal side of the lower eyelid and is frequently uncomfortable. Most cases are benign and resolve spontaneously with lifestyle improvements.
On the other hand, eyelid twitching may also hide more serious conditions such as essential blepharospasm or hemifacial spasm. These diseases have different pathologies from orbicularis myokymia and require appropriate diagnosis and treatment.
Orbicularis myokymia can occur in anyone regardless of age or sex. The prevalence of essential blepharospasm is reported as about 16–133 per 100,000 people1), and it is more common in middle-aged and older women. The prevalence of hemifacial spasm is about 10 per 100,0002). Essential blepharospasm is chronic and progressive, with symptoms advancing in the first 5 years, then often stabilizing. While 10% experience remission, 15% progress to functional blindness.
2. Types and differential diagnosis of eyelid twitching
Orbicularis oculi myokymia occurs in a limited part of the orbicularis oculi muscle in one eye, and unlike essential blepharospasm, it is not accompanied by synchronous eyebrow depression. Essential blepharospasm is bilateral, often with increased blinking, photophobia, and dry eye sensation. It worsens in bright places, with fatigue, or during reading, and improves in dark places, during sleep, or with pressure on the eyebrow area (sensory trick). Hemifacial spasm typically starts from the lower eyelid and gradually spreads to the entire facial muscles.
Orbicularis Oculi Myokymia (Benign Twitching)
Symptoms: Twitching of the lower eyelid in one eye
Features: Only a limited part of the orbicularis oculi muscle moves, and it does not lead to difficulty opening the eye
Course: Resolves spontaneously within days to weeks. Early improvement can be expected by removing triggering factors
Essential Blepharospasm (Requires Medical Attention)
Symptoms: Repeated episodes of forced closure of both eyes
Features: Accompanied by drooping of the eyebrows, chronic and progressive, spontaneous recovery is rare
Course: Botulinum toxin type A injections are effective in 90% of cases. Regular treatment is necessary
Symptoms: Spasms spreading from one eyelid to the corner of the mouth and facial muscles
Features: Persists even during sleep. MRI/MRA is needed to confirm vascular compression
Course: Botulinum toxin is the first-line treatment. MVD can offer a cure
QIf eyelid twitching does not stop, which department should be consulted?
A
First, consult an ophthalmologist. If it is orbicularis oculi myokymia, you can receive advice on lifestyle improvements. If blepharospasm or hemifacial spasm is suspected, you may be referred to a neurologist or neurosurgeon. Especially in cases requiring bilateral eyelid closure attacks, spread of spasms to the corner of the mouth, or detailed brain examination by MRI, a specialized medical system in collaboration with ophthalmology is required.
3. Causes and Treatments of Orbicularis Oculi Myokymia
Orbicularis oculi myokymia is caused by hyperactivity of the facial nerve, and in most cases it results from transient triggering factors. Rarely, pontine lesions may be present, but the majority of cases encountered in daily practice are due to lifestyle issues.
It often improves with physical and mental rest, and sedatives may be used. The following self-care measures are fundamental.
In many cases, symptoms resolve naturally within days to weeks with lifestyle improvements. However, if symptoms persist for more than 2–3 weeks or affect both eyes, an eye examination is recommended.
QWill reducing coffee stop eyelid twitching?
A
Excessive caffeine is one trigger for orbicularis myokymia, and limiting it may improve symptoms 3). However, causes are often multifactorial, and it is important to also address lack of sleep, stress, and eye strain. If symptoms do not improve within 1–2 weeks after reducing caffeine or if they worsen, see an eye doctor.
4. When to See a Doctor (Distinguishing Benign Essential Blepharospasm and Hemifacial Spasm)
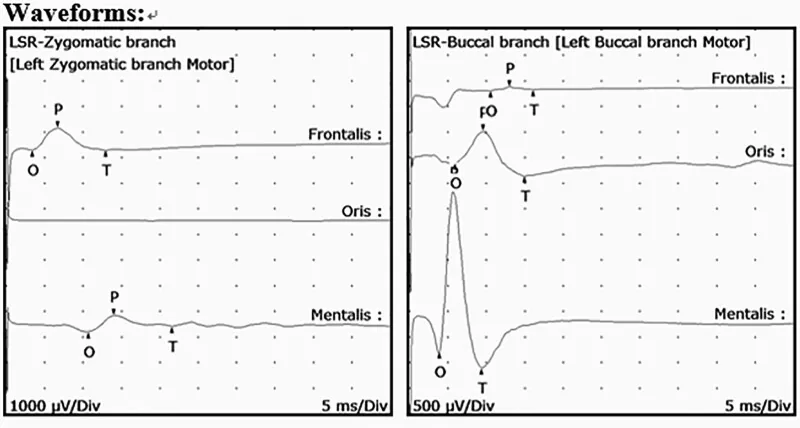
Ahn K, Jin Kim Y, Jung TY, Moon KS, Kim IY, Jung S. Strategy for dealing with unfamiliar and thick vessels during microvascular decompression: A first case report of hemifacial spasm caused by a persistent primitive trigeminal artery. Medicine (Baltimore). 2023;102(47):e36175. doi:10.1097/MD.0000000000036175. PMID:38013273. PMCID:PMC10681586. Figure 2. License: CC BY.
When stimulating the zygomatic and buccal branches of the facial nerve, abnormal electromyographic responses (lateral spreading response) spreading to the frontalis and mentalis muscles beyond the facial nerve territory are recorded. This corresponds to the electrophysiological diagnosis of hemifacial spasm discussed in section “4. When to see a doctor”.
The blink test is useful for diagnosing essential blepharospasm4). Severity is assessed in three stages: the rapid blink test (continue light, rapid blinking for 10–30 seconds), the gentle blink test (check whether blinking becomes impossible when the eyebrows move during voluntary blinking), and the forced blink test (repeat forced eyelid closure and check whether opening becomes impossible). In essential blepharospasm, rapid and gentle blinking become irregular, and eventually eyelid opening becomes difficult or impossible.
For diagnosing hemifacial spasm, confirm that synchronous spasms in the eyelid and mouth corner are induced by maneuvers such as repeated forced eyelid closure or lateral pulling of the mouth corner. MRI/MRA is used to identify compressive causes in the posterior cranial fossa (basilar artery, anterior inferior cerebellar artery, tumor, aneurysm, etc.).
Secondary blepharospasm includes extrapyramidal disorders such as Parkinson’s disease and progressive supranuclear palsy, chronic use of psychotropic drugs, and reflex blepharospasm due to local ocular irritative lesions such as keratitis, blepharitis, entropion, and iritis. Whether symptoms improve with local treatment also helps in differentiation.
Botulinum toxin type A suppresses acetylcholine release at nerve terminals, relaxing the overcontracted orbicularis oculi muscle. The efficacy rate of subcutaneous botulinum toxin type A injection for essential blepharospasm is 90%. The effect has a latency of 2–3 days after injection and lasts 3–4 months, requiring regular reinjections. In rare cases where patients develop blocking antibodies to type A, type F toxin may be used, but its duration is even shorter. Long-term safety and efficacy have been widely confirmed 5).
For hemifacial spasm, botulinum toxin therapy is also the first-line treatment, controlling symptoms with regular injections. As a curative treatment, posterior fossa microvascular decompression (MVD) is highly effective and can achieve long-term symptom resolution 6).
Lorazepam, clonazepam, and trihexyphenidyl may be used (all off-label). However, the effect varies greatly among individuals, with a response rate of only about 15%. Collaboration with an experienced neurologist is necessary.
When botulinum toxin is ineffective or insufficient, partial resection of the facial nerve (Reynold method) or resection of the orbicularis oculi muscle (Anderson method, protractor myectomy) may be considered. Surgical treatment is an option after adequate trials of botulinum toxin therapy.
QCan botulinum injections be received at an ophthalmology clinic?
A
Injection of botulinum toxin type A requires a registered physician system and can be performed at some ophthalmology facilities. Some facilities may require a referral, so first consult your regular eye doctor. After diagnosis and severity assessment of blepharospasm, you may be referred to a specialized facility that can administer botulinum toxin injections.
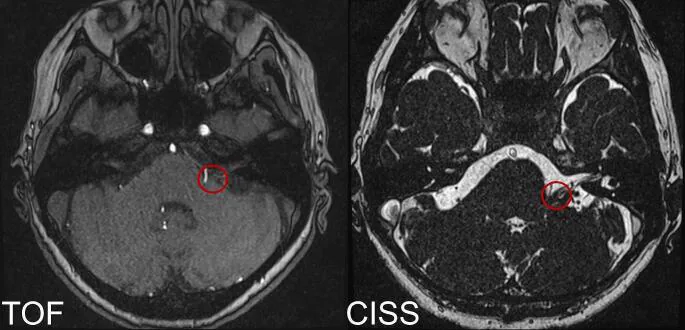
Falcone MM, et al. High-resolution MRI delineation of neurovascular conflict in hemifacial spasm. Acta Neurochir (Wien). 2024;166(1):239. Figure 1. PMCID: PMC11139744. License: CC BY.
Preoperative axial TOF (left) and CISS (right) MRI images show a suspected site of neurovascular compression (red circle) between the posterior inferior cerebellar artery (PICA) and the facial nerve at the root exit zone (REZ) near the brainstem surface. This corresponds to the mechanism of vascular compression of the facial nerve in hemifacial spasm discussed in section “6. Pathophysiology.”
Direct cause is hyperfunction of the facial nerve, leading to excessive discharge in a localized area of the orbicularis oculi muscle. Although there are reports of underlying pontine lesions, most cases encountered in daily practice are due to transient factors such as fatigue, stress, or caffeine. It resolves spontaneously when the hyperexcitability at the neuromuscular junction subsides.
Classified as a focal dystonia, it is thought to involve dysfunction of the basal ganglia. In normal blinking, the eyelid protractors (orbicularis oculi, corrugator supercilii, procerus) and retractors (levator palpebrae superioris, frontalis) are simultaneously inhibited. In essential blepharospasm, this reciprocal inhibition between the two muscle groups is lost. As a result, the eyelid-closing muscles contract intermittently or persistently, leading to repeated involuntary eyelid closure. An association with dopamine system dysfunction has also been reported7).
The following three pharmacological hypotheses have been proposed:
Cholinergic excess hypothesis: overactivity of cholinergic nerves
In the posterior cranial fossa, blood vessels such as the basilar artery or anterior inferior cerebellar artery, and rarely tumors or aneurysms, compress the facial nerve or pons. This sustained mechanical stimulation is thought to cause abnormal discharges in the facial nerve, leading to synchronous spasms via ephaptic transmission within the nerve. Identifying the compressing vessel through brainstem imaging (MRI/MRA) is key to diagnosis.
DaxibotulinumtoxinA (DaxibotulinumtoxinA for Injection) is a novel type A botulinum toxin preparation using a peptide excipient, expected to have a prolonged duration (about 6 months). A phase 2 trial for cervical dystonia showed dose-dependent efficacy 8), and research is ongoing for its application to blepharospasm.
Research on deep brain stimulation for refractory dystonia is advancing. Stereotactic thalamotomy targeting the ventral oral nucleus (Vo) has been reported in retrospective studies to have high long-term efficacy for focal dystonia including hand dystonia 9). Application of DBS to blepharospasm is currently limited, but research continues as an option for refractory cases.
Microvascular decompression (MVD) for hemifacial spasm is a curative treatment with high long-term success rates 6), and endoscopic-assisted MVD is advancing toward less invasiveness. Endoscopy expands the view of the cerebellopontine angle and is said to improve the accuracy of identifying the compressing vessel 10).
Improving QOL through Multidisciplinary Collaboration
Blepharospasm and hemifacial spasm cause not only visual dysfunction but also a wide range of QOL impairments, including difficulty working, social phobia, and depressive symptoms. The usefulness of multidisciplinary team care (ophthalmology, neurology, neurosurgery, psychiatry, rehabilitation) has been pointed out11), and establishing a system to support patients’ return to society and improve their daily quality of life remains a challenge.
Fred G. Barker, Peter J. Jannetta, David J. Bissonette, Philip T. Shields, Mark V. Larkins, Hae Dong Jho. Microvascular decompression for hemifacial spasm. Journal of Neurosurgery. 1995;82(2):201-210. doi:10.3171/jns.1995.82.2.0201.
Hallett M. Blepharospasm: recent advances. Neurology. 2002;59(9):1306-12. doi:10.1212/01.wnl.0000027361.73814.0e. PMID:12434791.
Jankovic J, Truong D, Patel AT, Brashear A, Evatt M, Rubio RG, et al. Injectable DaxibotulinumtoxinA in Cervical Dystonia: A Phase 2 Dose-Escalation Multicenter Study. Movement disorders clinical practice. 2018;5(3):273-282. doi:10.1002/mdc3.12613. PMID:30009213; PMCID:PMC6032882.
Horisawa S, Ochiai T, Goto S, Nakajima T, Takeda N, Fukui A, et al. Safety and long-term efficacy of ventro-oral thalamotomy for focal hand dystonia: A retrospective study of 171 patients. Neurology. 2019;92(4):e371-e377. doi:10.1212/WNL.0000000000006818. PMID:30587520; PMCID:PMC6345121.
Sindou M, Mercier P. Microvascular decompression for hemifacial spasm : Surgical techniques and intraoperative monitoring. Neuro-Chirurgie. 2018;64(2):133-143. doi:10.1016/j.neuchi.2018.04.003. PMID:29784430.
Castelon Konkiewitz E, Trender-Gerhard I, Kamm C, et al. Service-based survey of dystonia in Munich. Neuroepidemiology. 2002;21(4):202-206. doi:10.1159/000059525.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.