A general term for ocular and structural complications that occur after cosmetic eyelid surgery, such as double-eyelid surgery (blepharoplasty), eyelid fat removal, and ptosis correction.
Cosmetic eyelid surgery is one of the most common procedures in plastic surgery and includes double-eyelid surgery (suture and incision methods), eyelid fat removal (upper and lower eyelids), and ptosis correction for cosmetic purposes. Although surgical techniques have improved, complications still occur at a certain rate, and ophthalmic evaluation is essential for diagnosis and management2).
Complications are classified by when they appear into early complications (within a few weeks after surgery) and late complications (after several months to years). Early complications include infection, hematoma, suture abscess, overcorrection, and undercorrection; late complications include ptosis, incomplete eyelid closure, irregular double-eyelid crease, ectropion, upper eyelid hollowing (hollow eye) due to excessive orbital fat removal, worsening dry eye, scars, and keloids2,5).
Patients who had surgery in a cosmetic clinic may visit ophthalmology or oculoplastic surgery because of complications. As an ophthalmologist, one must be able to diagnose these complications appropriately and decide between conservative treatment, surgical revision, or referral to another department2).
QWhat kinds of problems can occur after cosmetic eyelid surgery?
A
In the early period (within a few weeks after surgery), infection, hematoma, suture abscess, overcorrection (lagophthalmos, where the eyes do not close well), or undercorrection (loss of the double-eyelid crease or asymmetry) may occur. In the late period (months to years later), ptosis, chronic lagophthalmos, an irregular double-eyelid crease, superior eyelid hollowing (hollow eye) from excessive orbital fat removal, and worsening dry eye may occur.
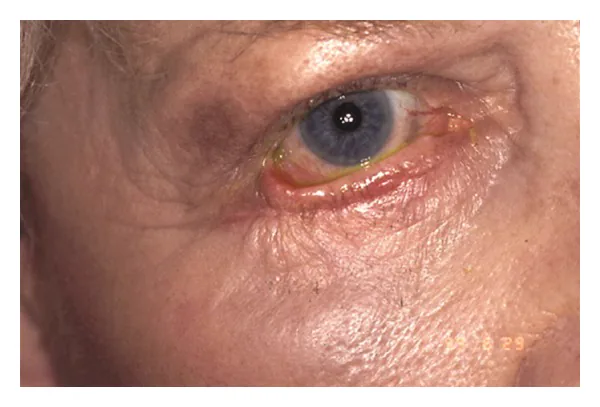
Oestreicher J, Mehta S. Complications of Blepharoplasty: Prevention and Management. Plast Surg Int. 2012;2012:252368. DOI: 10.1155/2012/252368. Figure 4. License: CC BY 3.0. PMCID: PMC3357590.
Clinical findings of cicatricial ectropion, in which the lower eyelid margin is pulled markedly downward and outward, the tarsal conjunctiva is broadly exposed and red, and much of the sclera is exposed. This corresponds to the ectropion discussed in the section “Classification and symptoms of complications” (anterior lamellar traction due to cicatricial contracture).
2-1. Early complications (within a few weeks after surgery)
hardening, pus drainage, and foreign-body sensation
foreign-body reaction to the buried suture
overcorrection
immediately after surgery to several weeks later
widened eyelid opening, incomplete eyelid closure, and corneal dryness
excessive removal of skin and muscle
Undercorrection
Immediately after surgery to several weeks
Loss or asymmetry of the eyelid crease
Insufficient fixation and suture loosening
Infection causes redness, swelling, pain, and fever, and if it progresses to orbital cellulitis it requires urgent treatment. A hematoma can occur early after surgery when hemostasis is insufficient, and a large hematoma can compress the optic nerve and cause vision loss5). A suture abscess is caused by a foreign-body reaction to the thread used in buried-suture methods, and suture removal is the definitive treatment2).
Overcorrection occurs when too much skin and orbicularis oculi muscle are removed, making the palpebral fissure too large and causing inability to close the eyelids. If eyelid closure failure persists, the cornea can dry out, increasing the risk of exposure keratitis (lagophthalmos keratopathy). Undercorrection occurs when double-eyelid fixation is insufficient, causing the crease to disappear or become asymmetric.
Ptosis can occur because of levator aponeurosis injury during surgery or postoperative scar contracture. Lagophthalmos results from excessive removal of the skin and orbicularis oculi muscle, leaving too little tissue needed for eyelid closure. Hollow eye (upper eyelid hollowing) is a depression of the upper eyelid caused by excessive removal of orbital fat, which creates a cosmetic problem and may also be accompanied by enophthalmos1).
Ectropion occurs due to outward traction from excessive removal of the anterior lamella (skin and orbicularis oculi) and scar contracture, and it causes tearing and corneal damage. Entropion is caused by traction on the posterior lamella from sutures or adhesions 2).
QWhy can it become hard to close the eyes after cosmetic surgery?
A
Closing the eyelids requires contraction of the orbicularis oculi muscle and enough skin. If too much skin and orbicularis muscle is removed during double-eyelid surgery or eyelid fat removal, there is not enough tissue needed for closure, and the eye cannot close completely (lagophthalmos). If lagophthalmos persists, the cornea can dry out, raising the risk of exposure keratitis. The eye surface is protected with artificial tears and eye ointment, and severe cases may require skin grafting.
Cosmetic eyelid surgery is one of the most commonly performed groups of procedures in cosmetic surgery. Double-eyelid surgery (buried-suture and incisional methods) is performed especially widely in Asia, including Japan, and is carried out in large numbers mainly at cosmetic surgery clinics.
Systematic data on the exact frequency of complications are limited. Minor complications of blepharoplasty (mild dry eye, chemosis, granuloma, ptosis, and scleral exposure) have been reported as relatively common 2), and most of these are considered recoverable with appropriate care.
Among complications after procedures performed in cosmetic surgery clinics, correction of ptosis, treatment of lagophthalmos, and correction of hollow eye are issues. In cases with corneal damage or eyelid malposition, coordination between cosmetic surgeons and ophthalmology/oculoplastic surgery is important 5).
In diagnosing complications after cosmetic eyelid surgery, taking a detailed surgical history is most important. Confirm the procedure used (buried-suture method, incisional method, whether fat was removed), the timing of surgery, the operator, and the postoperative course. If preoperative photos are available, they are useful for comparison with the preoperative state.
Examination item
Purpose
Method / evaluation
MRD-1 measurement
Eyelid position assessment
Distance from the corneal light reflex to the upper eyelid margin (normal 4–5 mm). Compare with preoperative photos
Levator function test
Assessment of levator aponeurosis injury
Excursion of the eyelid margin from down gaze to up gaze (normal ≥ 15 mm)
Fluorescein corneal staining
Assessment of the severity of corneal damage
Check for the pattern of epithelial damage caused by incomplete eyelid closure
Slit-lamp examination
Check for retained suture and inflammation
Detailed observation of the anterior segment, and whether sutures or corneal damage are present
Schirmer test and tear break-up time (BUT) measurement
MRD-1 (margin reflex distance 1) is the distance from the corneal light reflex at the center of the cornea to the upper eyelid margin, and it allows objective evaluation of eyelid position. Normally it is 4–5 mm, and if it is reduced after surgery, it suggests a complication of ptosis3).
In the levator function test, the distance the eyelid margin moves from downward gaze to upward gaze is measured. If levator function is preserved (≥ 15 mm), the prognosis after levator aponeurosis refixation is good, and this is used to help choose the surgical method.
In evaluating lagophthalmos, the remaining palpebral fissure width is recorded in mm during forceful voluntary closure, gentle closure, and blinking. Observation in the supine position is also important, because lagophthalmos may become more noticeable than in the sitting position. If sleep-related lagophthalmos is suspected, family members should be asked to take photos of the eyes during sleep.
With fluorescein staining, corneal epithelial damage associated with lagophthalmos has a characteristic pattern of segmental involvement in the lower part. The extent and depth of epithelial damage in the lower cornea are assessed, and treatment is chosen according to severity.
QIf a complication occurs after cosmetic eyelid surgery, where should I go for care?
A
Visiting an ophthalmologist or oculoplastic surgeon is recommended. Even if the surgery was performed in a cosmetic surgery clinic, ophthalmic examinations such as MRD-1 measurement and corneal staining are needed to assess corneal damage from lagophthalmos and ptosis. At the visit, bringing information about the procedure, timing, and surgeon, as well as preoperative photos if available, allows for a more accurate evaluation.
For corneal damage caused by incomplete eyelid closure, protecting the ocular surface is the top priority.
Artificial tears: Instill sodium hyaluronate eye drops or similar products frequently (4 to 8 times a day or more)
Eye ointment: Apply an antibiotic eye ointment (such as ofloxacin eye ointment) before bedtime to protect the ocular surface and help keep the eye closed
Taping: After applying eye ointment at bedtime, tape vertically from the upper eyelid to the lower eyelid to help keep the eye closed
Eye patch / moisture chamber: Keep the area around the eye humid and reduce corneal dryness
Response to infection:
For infection and orbital cellulitis, use antibiotic eye drops and oral antibiotics (or intravenous administration). For a suture abscess, removing the suture is the curative treatment.
Inflammation control:
Steroid eye drops may be used for postoperative conjunctival edema (chemosis) and inflammation.
Infection and cellulitis: Antibiotic treatment. If an abscess forms, incision and drainage are needed.
Hematoma: Compression immediately after surgery. Large hematomas or cases with optic nerve compression require urgent drainage.
Suture abscess: For suture abscesses from the buried technique, suture removal is the definitive treatment.
Overcorrection (lagophthalmos): Mild cases are managed with observation and protection of the ocular surface. Moderate to severe cases may need corrective surgery with aponeurosis recession or skin grafting.
Surgical management of late complications
Ptosis: Levator aponeurosis refixation is the standard treatment. The aponeurosis is resutured to the tarsus.
Lagophthalmos: Reconstruction of the anterior lamella with a skin graft or flap. In severe cases, a full-thickness skin graft is needed.
Hollow eye: Fat injection or hyaluronic acid injection. Complete recovery may be difficult1).
Ectropion: Anterior lamellar skin grafting, ligament repair, and lateral canthopexy (lateral tarsal strip method). Entropion is treated with scar excision and suture removal.
In severe lagophthalmos (caused by overresection of the skin and orbicularis oculi muscle), corneal damage will progress with conservative treatment alone. The following corrective surgeries are performed.
Skin graft (full-thickness graft): Full-thickness skin taken from behind the ear or the inner upper arm is grafted to the overresected area
Flap (local flap): Adjacent skin is used to improve lagophthalmos
Aponeurosis recession: For lagophthalmos caused by overcorrection (widened palpebral fissure), the levator aponeurosis is recessed (relaxed)
For postoperative ptosis caused by injury to the levator aponeurosis, levator aponeurosis refixation is the standard treatment. The cut ends of the aponeurosis are identified and sutured again to the tarsal plate (the eyelid plate). It is also indicated for secondary ptosis due to postoperative scar contracture, but depending on the degree of scarring, aponeurosis advancement or a suspension procedure (frontalis sling method) may be needed.
The following are performed for upper eyelid hollowing (hollow eye) caused by overresection of orbital fat1).
Autologous fat injection: Fat taken from the abdomen or thigh is injected into the upper eyelid. The survival rate varies, and multiple injections may be needed
Hyaluronic acid injection: Has the advantage of immediate effect, but the effect is temporary (about 6 to 18 months) and periodic reinjection is needed
Orbital fat grafting: A method using orbital fat from another site has also been reported4)
Patients should be told that complete recovery may be difficult.
QCan Hollow eye (depression of the upper eyelid) be corrected?
A
For Hollow eye caused by overresection of orbital fat, fat injection or hyaluronic acid injection may be performed1). Fat injection uses the patient’s own tissue, so a natural result can be expected, but the take rate varies and multiple treatments may be needed. Hyaluronic acid injection works quickly, but the effect is temporary and periodic reinjection is required. Complete recovery may sometimes be difficult, and for prevention, careful judgment of the amount of fat removed in the initial surgery is most important.
To prevent complications of cosmetic eyelid surgery, thorough preoperative ophthalmic evaluation and careful choice of procedure are essential.
Preoperative ophthalmic evaluation:
MRD-1 measurement: Record the preoperative eyelid position and use it for comparison after surgery
Levator function test: Understand function when there is no levator aponeurosis damage
Dry eye evaluation (Schirmer test and BUT): Identify existing dry eye and incomplete eyelid closure. Preoperative dry eye is a risk factor for worsening after surgery
Eyelid closure evaluation: Record the preoperative closure status and use it as the baseline for risk of overcorrection
Careful selection of the surgical procedure:
Careful judgment of skin excision: keep removal of the orbicularis oculi muscle and skin to a minimum, and avoid overresection
Limit fat removal: overresection of orbital fat is the main cause of hollow eye, so keep the amount removed conservative
Assess indications for buried-suture vs incisional methods: choose the appropriate procedure according to the degree of skin laxity and the condition of the tarsal plate
Informed consent:
Before surgery, fully explain the risks of complications (incomplete eyelid closure, ptosis, hollow eye, etc.). Especially in patients with dry eye, the risk of worsening dry eye after surgery is higher, and eye drop treatment may sometimes be started before surgery 2).
Collaboration between cosmetic surgery and ophthalmology/oculoplastic surgery:
It is desirable for cosmetic surgery facilities to have a collaborative system with ophthalmology or oculoplastic surgery that can perform ophthalmic evaluation and manage complications. If a complication occurs, establish a system for appropriate referral to ophthalmology or oculoplastic surgery.
The levator palpebrae superioris attaches to the tarsal plate via the levator aponeurosis and is responsible for opening the eye. In cosmetic eyelid surgery, especially incisional double-eyelid surgery, this aponeurotic part may be directly injured by surgical manipulation.
Direct injury: cutting or thinning of the aponeurosis by a scalpel or electrocautery
Secondary scar contracture: postoperative inflammation→scar formation→scar contracture of the aponeurosis→aponeurotic rupture and dysfunction
Levator edema/hematoma: postoperative swelling may temporarily reduce levator function, and scarring may remain after recovery
Postoperative ptosis has been reported as a complication of blepharoplasty and is more likely to occur after upper eyelid surgery2).
Eyelid closure requires the contractile force of the orbicularis oculi muscle and a sufficient amount of the anterior lamella (skin and orbicularis oculi muscle).
Excess removal of skin and orbicularis oculi muscle: the amount of anterior lamella tissue needed for eyelid closure becomes insufficient. This occurs especially when too much skin is removed in incisional surgery
Scar contracture: postoperative scarring pulls the eyelid upward and causes a physical inability to close the eye
Associated ectropion: ectropion that develops after excess removal of the anterior lamella further worsens the inability to close the eye
Lagophthalmos → tear film breakdown → corneal dryness → epithelial damage (superficial punctate keratopathy) → epithelial defect → infection → corneal ulcer may progress in this order2).
The post-septal fat and pre-septal fat of the upper eyelid give the upper eyelid its full volume. If these orbital fat pads are overremoved:
Upper eyelid hollowing: a cosmetic problem in which the eyelid appears deeply sunken when viewed from the front
Enophthalmos: the eyeball is pulled backward due to a reduction in orbital volume (enophthalmos-like)
The most important preventive measure is making the correct decision about how much fat to remove during the first surgery, because correction after overresection is difficult4).
Morley AM, Malhotra R. Use of hyaluronic acid filler for tear-trough rejuvenation as an alternative to lower eyelid surgery. Ophthalmic Plast Reconstr Surg. 2011;27:69-74. doi:10.1097/iop.0b013e3181b80f93.
Pacella SJ, Codner MA. Minor complications after blepharoplasty: dry eyes, chemosis, granulomas, ptosis, and scleral show. Plastic and reconstructive surgery. 2010;125(2):709-718. doi:10.1097/PRS.0b013e3181c830c7. PMID:20124856.
Koka K, Zeppieri M, Vadeo A, Patel BC. Blepharoptosis (Ptosis): Classification, Evaluation, and Surgical Management. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Last Update: 2026 Apr 19. Bookshelf ID: NBK539828. https://www.ncbi.nlm.nih.gov/books/NBK539828/
Goldberg RA, Lessner AM, Shorr N, et al. The transconjunctival approach to the orbital floor and orbital fat: a prospective study. Ophthalmic Plast Reconstr Surg. 1990;6:241-246. doi:10.1097/00002341-199012000-00003.
Oestreicher J, Mehta S. Complications of blepharoplasty: prevention and management. Plast Surg Int. 2012;2012:252368. doi:10.1155/2012/252368.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.