Hemifacial spasm (HFS) is a movement disorder characterized by involuntary tonic-clonic contractions of the facial muscles on one side of the face (innervated by the seventh cranial nerve). The ICD-10 code is G51.3.
In 1905, Joseph Babinsky first used the term “hemifacial spasm” 9). In 1947, Campbell and Keedy first described primary HFS, and in 1975, Jannetta clarified the mechanism of nerve compression by a tortuous dilated artery.
The prevalence in the United States is estimated at 8 to 15 per 100,000 people. The incidence is reported to be approximately 0.78 per 100,000 person-years 2). Another US report gives a prevalence of 11 per 100,000 3). Women are affected about twice as often as men, and the typical age of onset is 50 to 60 years, with a higher incidence in middle-aged and elderly individuals. The course is chronic and progressive.
Classification: It is broadly divided into primary (due to vascular compression) and secondary (due to abnormal regeneration after nerve injury or inflammation, tumors, demyelinating diseases, etc.).
Main differential diagnoses:
Eyelid myokymia: Involves only a part of the orbicularis oculi muscle and does not lead to difficulty opening the eye. It is not accompanied by synchronous eyebrow depression.
Blepharospasm (benign essential blepharospasm/BEB): Bilateral. Presumed basal ganglia dysfunction. Accompanied by photophobia and dry eye sensation, relieved by sensory tricks. Differs from HFS in that it disappears during sleep.
Meige syndrome: Bilateral blepharospasm that extends downward, accompanied by facial involuntary movements such as lip dyskinesia, a focal dystonia.
QHow is hemifacial spasm different from blepharospasm?
A
HFS is unilateral and extends to the lower face, with spasms persisting during sleep. Blepharospasm (BEB) is bilateral, centered around the orbits, accompanied by photophobia and dry eye sensation, and disappears during sleep. Tearing on the affected side is more common in HFS, while photophobia and dryness are less common in HFS.
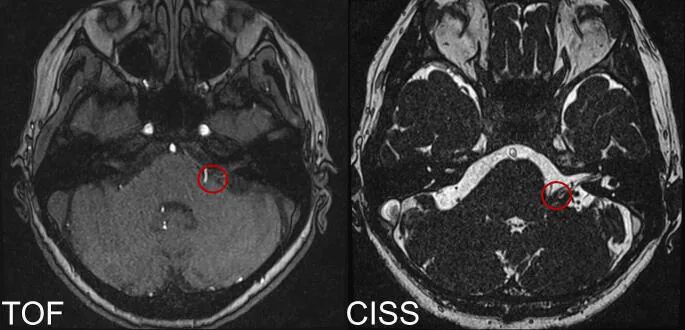
Rhomberg T, et al. Endoscope-assisted microvascular decompression in hemifacial spasm with a teflon bridge. Acta Neurochir (Wien). 2024. Figure 1. PMCID: PMC11139744. License: CC BY.
Preoperative axial TOF and CISS MRI sequences show possible contact (red circle) between the posterior inferior cerebellar artery (PICA) and the left facial nerve at the facial nerve root exit zone near the brainstem surface, corresponding to neurovascular compression discussed in section “2. Main symptoms and clinical findings”.
In the early stage, it often begins with mild twitching of the lower eyelid. Gradually, it spreads to the entire facial muscles including the eyelids, mouth corner, and platysma. Twitching of the eyelids and mouth corner occurs synchronously (same rhythm).
Onset: Involuntary contraction of the lower eyelid.
Progression: Intermittent eyelid twitching → sustained involuntary eye closure → spread to ipsilateral lower face and platysma.
Typical pattern: Starts from the upper and lower eyelids and spreads downward (most cases).
Atypical form: Begins in the orbicularis oris muscle and spreads upward (toward the eyelids).
Lacrimation: Often patients notice tearing on the affected side. Photophobia and dry eye sensation are less common (a distinguishing point from blepharospasm).
Triggers and exacerbating factors: Becomes more pronounced with emotional state and stress. Sleep disturbances associated with spasms may occur.
Continues during sleep: HFS is also observed during sleep (an important distinguishing point from blepharospasm).
Pulsatile tinnitus: May occur when the tensor tympani muscle is involved.
Clinical Findings (Findings Confirmed by Physician Examination)
Unilateral orbicularis oculi spasm: Synchronized with spasms of other facial muscles.
The other Babinski sign: Involuntary eyelid closure accompanied by brow elevation9).
Subtle facial muscle weakness: May be observed on the affected side.
Hearing loss: May be present.
Induction of synchronous spasms: Repetitive forced eyelid closure or lateral pulling of the mouth corner can induce synchronous spasms in the eyelid and mouth corner areas.
Inability to open the eyelid: Antagonism between spasm and effort to open the eyelid may lead to inability to open the eyelid, accompanied by relaxation of surrounding tissues.
QDoes hemifacial spasm occur during sleep?
A
HFS is also observed during sleep. This is an important distinguishing feature from blepharospasm. Blepharospasm disappears during sleep, but HFS continues during sleep.
Definition: Caused by vascular compression of the facial nerve at the root exit zone (REZ). The most common responsible vessel is the AICA (anterior inferior cerebellar artery).
The main cause is compression of the facial nerve and pons in the posterior cranial fossa by blood vessels such as the basilar artery or AICA, and rarely by tumors or aneurysms.
Risk factors: facial trauma, cranial nerve VII injury, history of Bell’s palsy, arteriosclerosis, family history. Aging and hypertension promote tortuous dilation of blood vessels, increasing the risk of associated syndromes (such as combination with trigeminal neuralgia)5).
Provocation test: Repetitive forced eye closure or pulling the corners of the mouth can induce synchronous spasms in the eyelid and mouth area, helping to confirm the diagnosis.
Imaging of the brainstem is important to determine the cause of compression.
MRI: High-resolution imaging along the facial nerve pathway from the cerebellopontine angle (CPA), internal auditory meatus (IAM), brainstem to the skull base exit is recommended. High-resolution T2-weighted imaging can visualize vascular compression, but asymptomatic neurovascular contact may also be seen in normal individuals.
3D-CISS MRI: Can depict the relationship between nerves and blood vessels in detail5).
3D-MRI fusion imaging (diffusion tensor imaging + magnetic resonance angiography): Useful for identifying the exact compression site at the REZ7).
Magnetic resonance angiography (MRA): In idiopathic intracranial hypertension-related HFS, vascular contact may not be seen 9).
Contrast-enhanced CT: An alternative when MRI cannot be performed.
AMR (abnormal muscle response)/LSR (lateral spread response): Essential for intraoperative monitoring during MVD. Disappearance of AMR can predict postoperative resolution of spasms 1)2).
Botulinum toxin type A (Botox(R) for injection) is covered by insurance in Japan for blepharospasm and hemifacial spasm. Currently, botulinum toxin therapy is considered the first-line treatment.
Mechanism of action: It is taken up by nerve terminals at the neuromuscular junction, acts on synaptic vesicle membrane proteins, and inhibits the release of acetylcholine.
Efficacy and duration:
Efficacy rate approximately 90%.
Onset of effect requires a latency of 2 to 3 days.
The effect lasts about 3–4 months (due to neuromuscular transmission resuming via sprouting of nerve collaterals). Repeated injections are necessary.
Long-term efficacy may decrease with high-dose frequent treatment.
Rarely, if blocking antibodies to type A toxin develop, type F toxin is effective (but with shorter duration).
Injection sites and doses: corrugator supercilii, orbicularis oculi (evenly distributed), zygomaticus major, levator labii superioris alaeque nasi. 2.5 units each. It is important to avoid accidental injection into the levator palpebrae superioris.
Carbamazepine, clonazepam, phenytoin, gabapentin, baclofen. Efficacy is limited and side effects are significant. For HFS associated with IIH, topiramate (50 mg twice daily) has been reported to be effective9).
QHow long does the effect of botulinum toxin last?
A
The effect lasts about 3 to 4 months. Because neuromuscular transmission resumes due to sprouting of nerve collaterals, repeated injections are needed when the effect wears off. High-dose or frequent treatment may lead to reduced long-term efficacy.
QWhich patients are suitable for microvascular decompression?
A
The main indications are refractory cases with poor response to botulinum toxin and younger patients. The improvement rate is about 90%, and long-term outcomes are good. In elderly patients without complications, results comparable to younger patients can be expected5).
6. Pathophysiology and Detailed Mechanism of Onset
The basic mechanism of primary HFS is vascular compression → demyelination → ephaptic transmission (false synaptic transmission). Electrical activity in one nerve induces activation of a neighboring nerve. The mechanism differs from blepharospasm involving the basal ganglia.
Vulnerable site of the facial nerve: The central myelin portion from the root exit point (RExP) to the transitional zone (TZ), about 10 mm, is vulnerable to vascular compression. The Obersteiner-Redlich zone (transition from central to peripheral myelin) within this portion is considered particularly vulnerable7).
Sano et al. (2022) evaluated pre- and post-MVD using 3D-MRI fusion images (DTI+MRA). They reported that the TZ of the facial nerve is approximately 0.96 mm (range 1.9–2.86 mm) and demonstrated that the AS portion of the REZ can be accurately identified 7).
Mechanism of double compression (DC type): In DC-type HFS, REZ decompression may trigger a “lever principle” that worsens compression on the CP side. Displacement of a thick atherosclerotic VA pushes up the AICA, exacerbating facial nerve compression at the CP portion 1).
Fujii et al. (2024) reviewed 35 cases of DC-type HFS and reported that when AMR does not disappear after REZ decompression, confirming AICA compression on the CP side and adding Teflon improves postoperative outcomes 1).
IIH-related HFS: Fluctuations in cerebrospinal fluid pressure (not absolute values but the amount of change) are thought to cause hyperexcitability of the facial nerve. This is supported by the induction of HFS attacks upon standing after lumbar puncture 9).
Combined HDS with trigeminal neuralgia: Occurs in approximately 3% of all HDS patients. Atherosclerotic vascular changes due to aging and hypertension cause elongation of blood vessels, compressing multiple adjacent nerves 5).
7. Latest Research and Future Prospects (Investigational Reports)
3D-MRI fusion imaging is useful for accurate depiction of the REZ and for preoperative simulation and postoperative evaluation. It can identify the cisternal segment of the facial nerve and visualize its positional relationship with the offending vessel 7).
With the introduction of dual-branch monitoring (facial nerve temporal branch stimulation → mentalis muscle recording + marginal mandibular branch stimulation → orbicularis oculi muscle recording), a 98% effectiveness rate after MVD has been reported 2). If AMR does not disappear, it is important to search for the responsible vessel outside the REZ (CP, IAC).
Guo et al. (2025) reported the first case of facial nerve compression by the labyrinthine artery within the IAC, demonstrating that dual-branch monitoring could detect IAC compression missed by conventional REZ exploration 2).
Vascular compression within the IAC, previously overlooked, can cause HFS. If AMR does not disappear, systematic exploration of the entire REZ → CP → IAC is necessary 2).
Pathophysiological Relationship Between IIH and HFS
A new pathophysiological concept has been proposed that cerebrospinal fluid pressure fluctuations can trigger HFS. Topiramate management of CSF pressure may be effective, and its application to the diagnosis and treatment of IIH-related HFS is attracting attention 9).
Fujii K, Mori K, Tamase A, Shima H, Nomura M, Yamamoto T. Dynamic changes of abnormal muscle response during decompression procedures in double compression-type hemifacial spasm. Surgical neurology international. 2024;15:430. doi:10.25259/SNI_768_2024. PMID:39640305; PMCID:PMC11618637.
Guo Z, Zhang X, Zhao B. Hemifacial spasms caused by compression of the labyrinthine artery on the facial nerve in the internal auditory canal: a case report and review of the literature. Journal of medical case reports. 2025;19(1):514. doi:10.1186/s13256-025-05285-0. PMID:41102849; PMCID:PMC12532876.
Guerrero J, Huang M, Britz G. Double Crush Syndrome as a Cause of Hemifacial Spasm. Cureus. 2021;13(1):e12448. doi:10.7759/cureus.12448. PMID:33552766; PMCID:PMC7853293.
Takaki Y, Tsutsumi S, Teramoto S, Nonaka S, Okura H, Suzuki T, et al. Quadrigeminal cistern arachnoid cyst as a probable cause of hemifacial spasm. Radiology case reports. 2021;16(6):1300-1304. doi:10.1016/j.radcr.2021.02.061. PMID:33854668; PMCID:PMC8026915.
Argie D, Lauren C, Malelak EB. A Rare Combined Trigeminal Neuralgia with Hemifacial Spasm in a 78-year-old Male Patient. Asian journal of neurosurgery. 2021;16(3):630-633. doi:10.4103/ajns.AJNS_433_20. PMID:34660385; PMCID:PMC8477817.
Liu Y, Chen F, Li Z, et al. Microvascular decompression and aneurysm clipping for a patient with hemifacial spasm and ipsilateral labyrinthine artery aneurysm. CNS Neurosci Ther. 2022;28:307-309.
Sano K, Kuge A, Kondo R, Yamaki T, Nakamura K, Saito S, et al. Ingenuity using 3D-MRI fusion image in evaluation before and after microvascular decompression for hemifacial spasm. Surgical neurology international. 2022;13:209. doi:10.25259/SNI_1015_2021. PMID:35673670; PMCID:PMC9168332.
Onoda K, Sashida R, Fujiwara R, Wakamiya T, Michiwaki Y, Tanaka T, et al. Intermediate nerve neuralgia developed during hemifacial spasm follow-up: illustrative case. Journal of neurosurgery. Case lessons. 2022;3(25):CASE22144. doi:10.3171/CASE22144. PMID:35733844; PMCID:PMC9210264.
Petersen GC, Amirkhizi M, Brockmann K, Dibaj P. Hemifacial spasm through changes of cerebrospinal fluid pressure in idiopathic intracranial hypertension. Proceedings (Baylor University. Medical Center). 2023;36(1):114-115. doi:10.1080/08998280.2022.2119544. PMID:36578612; PMCID:PMC9762843.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.