This refers to side effects that arise from systemic absorption of eye drops used to treat glaucoma. Although eye drops are applied locally to the eye, much of the solution reaches the nasal mucosa through the nasolacrimal duct after instillation and is absorbed into the systemic circulation.
About 80% of a single eye-drop dose (approximately 25–50 μL) drains into the nasolacrimal duct and can be absorbed through the nasal mucosa and gastrointestinal tract1). Because absorption from the nasal mucosa is not subject to first-pass hepatic metabolism, some drugs (especially β-blockers) can reach systemic blood levels equal to or higher than those seen with oral administration1).
In older patients with glaucoma, cardiovascular and respiratory comorbidities are common, so the risk of side effects is higher2). With combination drugs, it is also easy for patients not to realize that they are using eye drops that contain a β-blocker.
Drug classes for which systemic side effects are a concern
β-blockers (timolol, carteolol, levobunolol, etc.): the class that can cause the most serious systemic side effects
Alpha-2 agonists (brimonidine): risk of central nervous system depression in infants and young children
Oral carbonic anhydrase inhibitors (acetazolamide): metabolic acidosis and urinary stones
Prostaglandin preparations (latanoprost, travoprost, etc.): few systemic side effects
ROCK inhibitors (ripasudil): systemic side effects are rare
QCan eye drops cause side effects throughout the body?
A
About 80% of eyedrops drain into the nasolacrimal duct and are absorbed into the systemic circulation from the nasal mucosa1). Because absorption from the nasal mucosa does not undergo first-pass hepatic metabolism, beta-blockers in particular can reach relatively high blood concentrations. In patients with heart or respiratory disease and in infants, they can cause serious side effects.
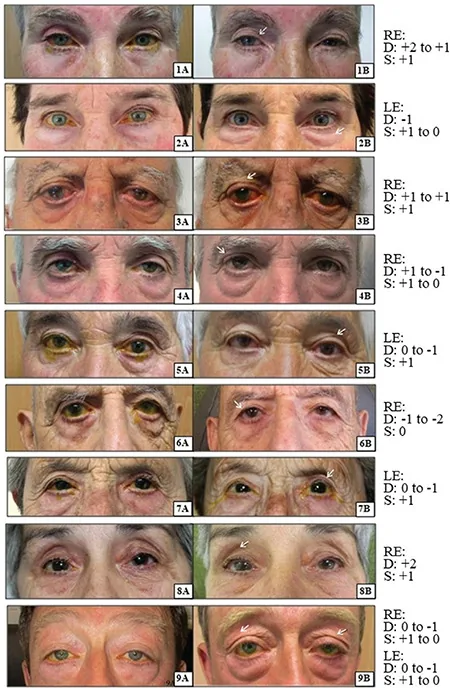
McCartney MH, Sammouh FK, Tong JY. Severe Microbial Keratitis Secondary to Prostaglandin-Associated Periorbitopathy. Case Rep Ophthalmol Med. 2025;2025:5635118. Figure 1 and Figure 2. PMID: 41103282; PMCID: PMC12527608. DOI: 10.1155/crop/5635118. License: CC BY 4.0.
Clinical photo showing the appearance around the eyes before stopping prostaglandin preparations (PGA) (panel A) and 1 year after stopping (panel B). The upper eyelid’s sunken appearance indicated by the arrows (deepening of the upper eyelid sulcus: DUES) and orbital periocular fat atrophy can be seen to improve after stopping. This corresponds to the local side effects of prostaglandin preparations (orbital fat atrophy and deepening of the upper eyelid sulcus) discussed in the “Symptoms and side effects by drug class” section.
The systemic side effects of each drug class are shown below.
Beta-blockers
Cardiovascular system: bradycardia, arrhythmia, worsening heart failure. One drop of timolol 0.5% eye drops can reach blood concentrations equivalent to 5–10 mg taken orally3).
Respiratory system: bronchoconstriction can worsen asthma and COPD. Due to beta2-receptor blockade.
Central nervous system: depression, fatigue, insomnia, nightmares, sexual dysfunction3).
Metabolic: masking of hypoglycemia (in patients with diabetes) and effects on lipid metabolism.
Prostaglandin analogues
Systemic side effects: Few. The frequency of systemic side effects is lower than with other drug classes.
Rare systemic symptoms: Reports of headache and muscle pain4).
Mainly local side effects: Periocular pigmentation, iris pigmentation, deepening of the upper eyelid sulcus, and eyelash growth4).
Notable examples: latanoprost, travoprost, tafluprost, and others.
Sulfonamide allergy: Cross-reactivity with sulfa drug allergy is rare5).
Oral medication (acetazolamide): numbness in the limbs, loss of appetite, metabolic acidosis, and urinary stones5).
Caution: Contraindicated in patients with a history of hypersensitivity to sulfonamides.
α2-agonists (brimonidine)
Systemic symptoms: Dry mouth, drowsiness, and fatigue. In older adults, somnolence and dizziness → be mindful of fall risk6).
Infants and newborns: Contraindicated: Because the blood-brain barrier is immature, there is a risk of central nervous system depression (respiratory depression, bradycardia, hypothermia, hypotension)6).
QCan glaucoma eye drops cause shortness of breath?
A
Beta-blocker eye drops block β2 receptors in the bronchi and can cause bronchoconstriction3). They are contraindicated in patients with asthma or COPD, and if you feel shortness of breath, wheezing, or difficulty breathing while using them, stop the drops immediately and consult your doctor. In an emergency, use a bronchodilator (such as isoproterenol).
3. Causes of systemic absorption and factors that increase risk
After instillation, the drug solution mixes with tears and flows into the nasal cavity through the puncta, canaliculi, and nasolacrimal duct1). The nasal mucosa is highly vascular and has a large absorption surface area, so the drug enters the systemic circulation directly without first-pass metabolism in the liver1). This route may be more efficient than oral administration, and some drugs can reach unexpectedly high blood concentrations.
Check the timing: Compare when the eye drops were started, changed, or increased with when the whole-body symptoms appeared
Dechallenge (stopping or changing the drug): If symptoms improve after stopping, a causal relationship is suggested
Rechallenge (readministration): Usually not needed. Careful judgment is required
Share information with internal medicine doctors and pharmacists: Systemic side effects from eye drops are easy to overlook2)
In older adults, systemic side effects from eye drops can be missed as a cause of fatigue, sleepiness, and depression-like symptoms2)6). In many cases, the internal medicine doctor does not know that glaucoma eye drops are being used, so using a medication notebook is helpful.
QCan glaucoma eye drops cause a decline in cognitive function?
A
Yes, it is possible. With β-blocker eye drops, fatigue and depression-like symptoms have been reported3). In older adults, these symptoms are especially easy to miss, and coordination with internal medicine and dementia specialists is important. Brimonidine (an α2 agonist) can also cause central nervous system side effects such as drowsiness and somnolence6).
If side effects occur, seek instructions from a specialist promptly. The following are emergency measures.
If bradycardia occurs: Intravenous atropine
Low blood pressure: Give sympathomimetics
Bronchial constriction: Use bronchodilators such as isoproterenol
If corneal epithelial damage or blepharitis is suspected: stop the beta-blocker and use only preservative-free hyaluronic acid preparations or artificial tears. Control intraocular pressure with oral acetazolamide
Patients with heart disease or asthma: avoid beta-blockers and prefer prostaglandin agents, alpha-2 agonists, and ROCK inhibitors8)
Beta1-selective drugs (betaxolol): may have less effect on lung function than non-selective drugs (timolol), but the risk cannot be completely avoided8)
Infants and young children: brimonidine is contraindicated. Consider prostaglandin agents and beta-blockers (use with caution) as alternatives6)
Harii K, Arase S, Tsuboi R, et al. Bimatoprost for Eyelash Growth in Japanese Subjects: Two Multicenter Controlled Studies. Aesthetic Plast Surg. 2014;38(2):451–460. Figure 1. Source ID: Wikimedia Commons / File:Bimatoprost_eyelash_growth.jpg. License: CC BY 4.0.
Clinical photograph showing eyelash hypertrichosis caused by bimatoprost eye drops (a prostaglandin-based medication). In subject A, the lashes changed from before treatment (GEA score 2: moderate) to 4 months later (GEA 4: very marked), and in subject B, from before treatment (GEA score 1: minimal) to 4 months later (GEA 2: moderate), showing lash lengthening and darkening. This corresponds to the local effects of prostaglandin agents (eyelash hypertrichosis and eyelash pigmentation) discussed in the section on “Pathophysiology and mechanisms of systemic absorption”.
As for pharmacokinetics after eye drop instillation, of the administered dose, no more than 5% passes through the cornea and reaches the intraocular tissues (anterior chamber and aqueous humor)1). Most of the rest is absorbed through the conjunctiva or drained through the nasolacrimal duct into the body.
Absorption from the nasal mucosa can bypass first-pass hepatic metabolism, so bioavailability may be higher than with oral administration1). With one drop of timolol 0.5% eye drops (about 50 μL, 250 μg), the amount absorbed systemically has been reported to reach blood concentrations equivalent to an oral dose of 5 to 10 mg3).
Nonselective β1/β2 beta-blockers act throughout the body through the following mechanisms.
Blockade of cardiac β1 receptors: reduced automaticity of the sinoatrial node → bradycardia and delayed atrioventricular conduction
Blockade of bronchial smooth muscle β2 receptors: bronchoconstriction → worsening of asthma and COPD
Effects on the central nervous system: partly crosses the blood-brain barrier and can cause depression, fatigue, and insomnia3)
Effects on metabolism: masking of the adrenaline response during hypoglycemia and abnormal lipid metabolism
β1-selective agents (betaxolol) have weaker action on β2 receptors and may have less effect on respiratory function than timolol in patients with asthma. However, this cannot be completely avoided8).
Brimonidine is an α2 receptor agonist that crosses the blood-brain barrier and stimulates central α2 receptors, producing sedative and hypotensive effects. In infants, the blood-brain barrier is immature, so central nervous system depression (altered consciousness, respiratory depression, bradycardia, hypothermia, and hypotension) is more likely to become severe, and it is considered contraindicated6). In older adults, it can also cause drowsiness and dizziness, increasing the risk of falls.
Measures such as lowering the dose, closing the eyes and pressing on the lacrimal sac after instillation, and sustained-release formulations are being studied to reduce systemic exposure1). The systemic side effect profiles of combination eye drops (such as prostaglandin/beta-blocker combinations) are also continuing to be evaluated2).
Research is progressing toward making eye drops unnecessary themselves. With DDS technologies such as sustained-release intraocular implants and microneedles, long-lasting drug effects are expected while avoiding systemic absorption9). This may lead to a fundamental solution to the problem of systemic side effects from eye drops.
Polypharmacy with eye drops and fall risk in older adults
Prospective studies on the risk of falls associated with the use of multiple glaucoma eye drops in older adults are being conducted6). Drowsiness, dizziness, and low blood pressure caused by brimonidine and beta-blockers may contribute to falls and fractures, and evaluation from a geriatric medicine perspective is needed.
A system has been reported that uses AI to integrate information such as a patient’s systemic comorbidities, medications, and kidney function to suggest the optimal glaucoma eye drops. From the standpoint of personalized medicine, it is expected to be applied to drug selection that minimizes the risk of side effects.
Urtti A, Salminen L. Minimizing systemic absorption of topically administered ophthalmic drugs. Survey of ophthalmology. 1993;37(6):435-56. doi:10.1016/0039-6257(93)90141-s. PMID:8100087.
Inoue K. Managing adverse effects of glaucoma medications. Clin Ophthalmol. 2014;8:903-913. PMID: 24872675. PMCID: PMC4025938. doi:10.2147/OPTH.S44708.
McMahon CD, Shaffer RN, Hoskins HD Jr, Hetherington J Jr. Adverse effects experienced by patients taking timolol. American journal of ophthalmology. 1979;88(4):736-8. doi:10.1016/0002-9394(79)90674-3. PMID:507146.
Alm A, Stjernschantz J. Effects on intraocular pressure and side effects of 0.005% latanoprost applied once daily, evening or morning. A comparison with timolol. Scandinavian Latanoprost Study Group. Ophthalmology. 1995;102(12):1743-1752. doi:10.1016/s0161-6420(95)30798-1.
Cimolai N. A review of neuropsychiatric adverse events from topical ophthalmic brimonidine. Hum Exp Toxicol. 2020;39(10):1279-1290. doi:10.1177/0960327120918307.
Tanihara H, Inoue T, Yamamoto T, Kuwayama Y, Abe H, Araie M, et al. Phase 2 randomized clinical study of a Rho kinase inhibitor, K-115, in primary open-angle glaucoma and ocular hypertension. American journal of ophthalmology. 2013;156(4):731-6. doi:10.1016/j.ajo.2013.05.016. PMID:23831221.
Dunn TL, Gerber MJ, Shen AS, Fernandez E, Iseman MD, Cherniack RM. The effect of topical ophthalmic instillation of timolol and betaxolol on lung function in asthmatic subjects. Am Rev Respir Dis. 1986;133(2):264-268. doi:10.1164/arrd.1986.133.2.264.
Kompella UB, Hartman RR, Patil MA. Extraocular, periocular, and intraocular routes for sustained drug delivery for glaucoma. Progress in retinal and eye research. 2021;82:100901. doi:10.1016/j.preteyeres.2020.100901. PMID:32891866; PMCID:PMC8317199.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.