
Synoptophore Examination
Key points at a glance
Section titled “Key points at a glance”1. What is a synoptophore examination?
Section titled “1. What is a synoptophore examination?”The synoptophore is a device mainly used for binocular function testing and training in strabismus, amblyopia, and eye movement disorders. Set at an optical distance equivalent to about 6 m, its greatest feature is that it can evaluate binocular visual function in detail while completely separating the right and left eyes.
Purpose of the test
Section titled “Purpose of the test”The main purposes of synoptophore testing are as follows.
- Assessment of simultaneous perception, fusion, and stereopsis: Quantitatively evaluates each of the three stages of binocular vision.
- Quantification of the strabismus angle: allows quantitative measurement of eye position in nine directions and measures both objective and subjective strabismus angles.
- Retinal correspondence testing: determines whether retinal correspondence is normal or abnormal.
- Measurement of fusion ranges: quantifies the width of the fusion range in the convergence and divergence directions.
- Quantification of torsional deviation: used to evaluate strabismus with a torsional component (such as superior oblique palsy).
- Amblyopia and strabismus training: amblyopia training using a pleoptic cover is possible.
The synoptophore is a device used for detailed evaluation and training of strabismus, amblyopia, and eye movement disorders. With the left and right eyes completely separated, it can evaluate simultaneous perception, fusion, and stereopsis; quantitatively measure the strabismus angle in nine directions; perform retinal correspondence testing (to determine normal or abnormal correspondence); measure fusion ranges; and quantify torsional deviation. It is also used for amblyopia training and strabismus training with a pleoptic cover. In routine clinical practice, it is widely used for pre- and postoperative evaluation of strabismus, quantitative assessment of binocular vision function, and fusion training (such as for convergence insufficiency).
2. Structure and principle of the device
Section titled “2. Structure and principle of the device”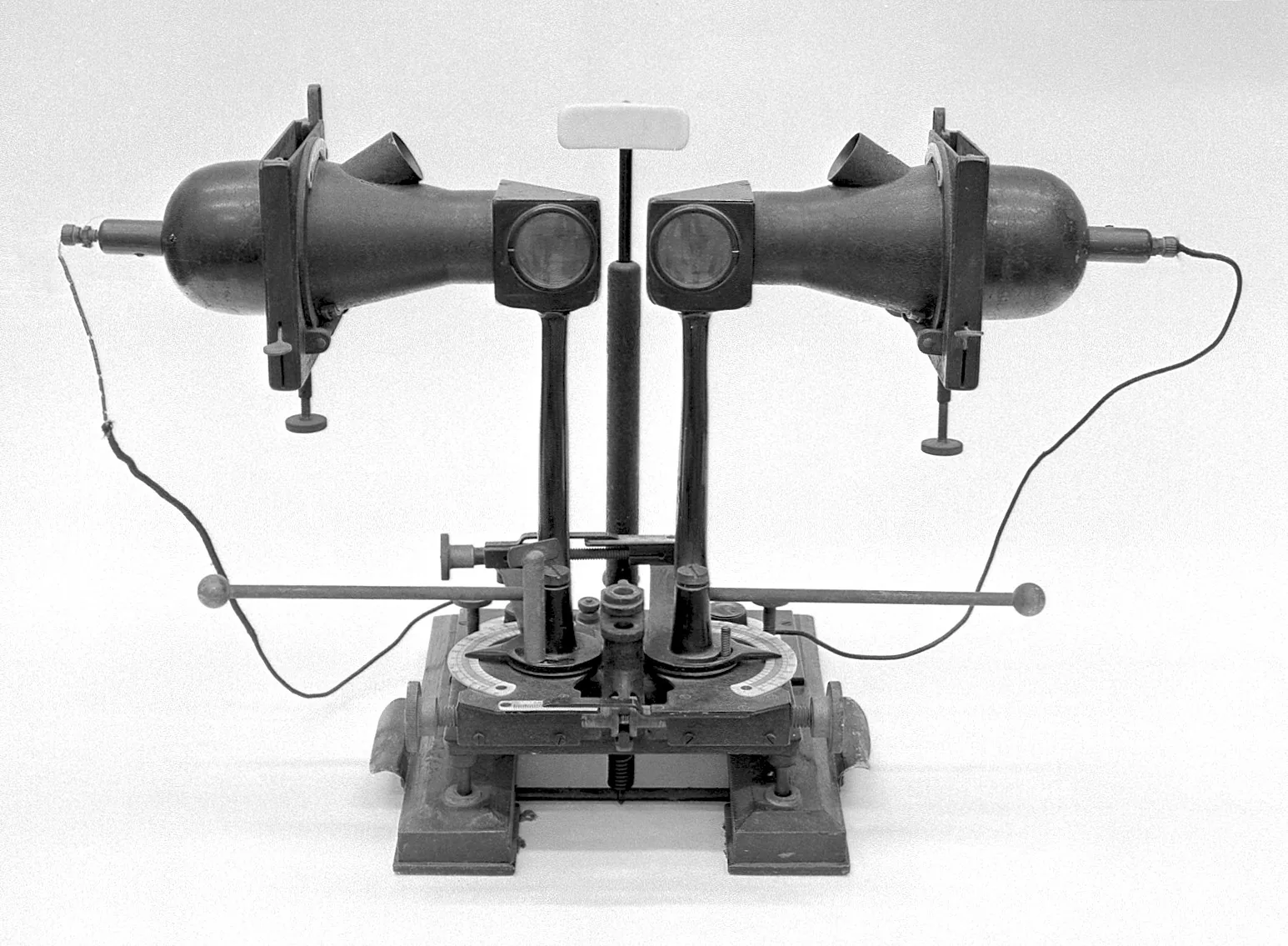
{kind=link}
The large amblyoscope consists of a tube body and angle display unit made up of a lighting chamber, slide chamber, reflector, and eyepiece section. The person being examined looks into the tube body and the examination is performed with the left and right eyes separated. Visual target slides can be inserted into the slide chamber at the tip of the tube body and presented as optical distant targets.
Main features of the device
Section titled “Main features of the device”- High binocular dissociation effect: The examination is performed with the left and right eyes completely separated. This strong dissociation, which is not available in everyday vision, makes suppression and anomalous correspondence easier to detect
- Nine gaze positions: The strabismus angle can be measured not only in the primary position but also in eight other gaze positions, making it suitable for evaluating paralytic and restrictive strabismus
- Slide exchange system: By changing the slides, it can be used for tests of simultaneous perception, fusion, stereopsis, retinal correspondence, and more
- Optical distance viewing (equivalent to 6 m): Examination can be performed without the influence of accommodation
- Both subjective and objective testing: Both objective measurement using corneal reflexes and subjective measurement based on the examinee’s report are possible
3. Types of examinations and procedure
Section titled “3. Types of examinations and procedure”Simultaneous vision test
Section titled “Simultaneous vision test”Use slides with different figures on the left and right (for example, a lion and a birdcage). Evaluate whether both figures can be recognized at the same time and confirm whether suppression is present. If different figures can be perceived simultaneously with both eyes, it is judged as having simultaneous vision. If one eye is suppressed, only one figure is seen.
Fusion test
Section titled “Fusion test”Use slides with the same figure on the left and right. Measure the range of angles at which the two images can be superimposed and seen as one (the fusion range). Quantify the width of the fusion range from the amount of inward and outward rotation of the instrument tubes. In children with intermittent exotropia, it has been reported that the convergence fusion width is lower than in healthy children 1. Note that the fusion range measured with the synoptophore and with a prism bar may not match (the synoptophore tends to show larger values, especially on the convergence side), so it is not recommended to use the two interchangeably 2.
The normal values for the fusion range are as follows.
- Abduction (convergence) direction: 5–10°
- Adduction (divergence) direction: 2–5°
Stereopsis test
Section titled “Stereopsis test”Slides with left-right disparity are used. This assesses whether depth perception is possible and confirms whether stereoscopic vision is present.
Retinal correspondence test
Section titled “Retinal correspondence test”The key point of retinal correspondence testing with a synoptophore is whether the objective strabismus angle matches the subjective strabismus angle. The test uses simultaneous-vision slides (figures with different shapes on the left and right).
| Assessment | Objective strabismus angle | Subjective strabismus angle | Interpretation |
|---|---|---|---|
| Normal correspondence | =Subjective strabismus angle | =Objective strabismus angle | Normal retinal correspondence |
| Comitant anomalous correspondence | ≠ subjective strabismus angle | 0° (sense of alignment present) | Anomalous correspondence is established |
| Incomitant anomalous correspondence | ≠ subjective strabismus angle | Other than 0° | Transient anomalous correspondence |
In general, test methods with stronger dissociation between the two eyes are more likely to detect deeper anomalous correspondence. The strong dissociation created by a synoptophore can reveal anomalous correspondence that may not be detected in tests closer to everyday vision. It has been reported that a technique in which the brightness of the synoptophore is gradually changed between the left and right sides can be used to quantify the depth of suppression with greater sensitivity than the Worth 4 Dot test3.
Quantifying the strabismus angle
Section titled “Quantifying the strabismus angle”The objective strabismus angle and the subjective strabismus angle are determined by the following methods.
- Objective strabismus angle: the angle when the tube is moved so that the corneal reflex comes to the foveal position. The examiner determines this by observing the corneal reflex from outside.
- Subjective strabismus angle: the angle at which the examinee feels the left and right targets overlap and look like one. Based on the examinee’s report.
The objective strabismus angle and the subjective strabismus angle are measured separately with a synoptophore, and the result is judged by comparing the two. The objective strabismus angle is determined by the examiner by observing the corneal reflex, and the subjective strabismus angle is the angle at which the examinee reports that the targets seem to overlap into one. If the two match (difference of 0), it is judged as normal correspondence. If they do not match, it is abnormal correspondence; if the subjective strabismus angle is 0° (there is a deviation in the strabismic eye but a sense of fusion remains), it is judged as harmonious anomalous correspondence, and if it is not 0°, it is judged as disharmonious anomalous correspondence.
4. Slide selection
Section titled “4. Slide selection”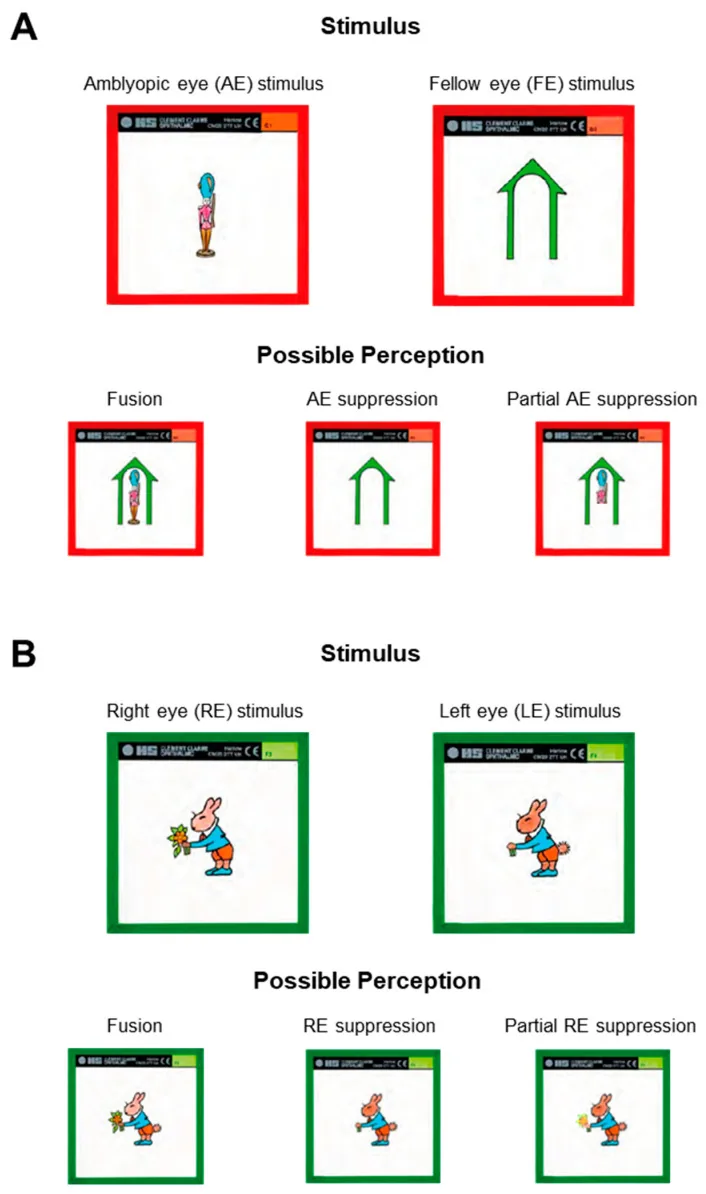
Several types of test slides are available as a paired set. It is important to choose the appropriate slide according to the purpose of the examination and the patient’s age.
| Slide type | Figure features | Main use |
|---|---|---|
| Slide for simultaneous perception | Different figures on the left and right (dissimilar figures) | Simultaneous perception test, retinal correspondence test |
| Fusion slide | Shapes that are almost the same in the left and right eyes (same-type figures, with differences created by fusion arrows) | Fusion range measurement |
| Stereopsis slide | Shapes with disparity between the left and right eyes | Stereopsis test |
| Slides for young children | Pictures such as animals and vehicles | Examination for young children |
The slides for young children use familiar pictures such as animals and vehicles, making them easier for preschool children to accept. There are also young-child versions for simultaneous perception, fusion, and stereopsis.
Comparison with other binocular vision tests
Section titled “Comparison with other binocular vision tests”There are several methods for binocular vision tests, and their characteristics vary depending on how strongly the eyes are separated and how close they are to everyday viewing distance.
| Test | Binocular dissociation | Distance from usual viewing | Ease of detecting suppression |
|---|---|---|---|
| Bagolini striated lenses | Weak | Close | Difficult to detect |
| Worth 4-dot test | Moderate | Moderate | Moderate |
| Synoptophore | Strong | Distant | Easy to detect |
| Afterimage test | Strongest | Farthest | Easiest to detect |
Generally, the stronger the binocular dissociation of a test, the more likely deep anomalous retinal correspondence is to be detected. With a synoptophore, anomalous retinal correspondence that is suppressed during everyday viewing may sometimes become apparent. On the other hand, because the results come from conditions far removed from everyday viewing, it is important to keep in mind that they may differ from binocular vision in actual daily life.
Bagolini striated lenses and the Worth 4-dot test are examinations performed under conditions close to everyday viewing, and they assess more practical binocular vision function. The synoptophore is suited to precise quantitative evaluation and training, and the two are used complementarily.
They are used according to the strength of binocular dissociation and how close they are to everyday viewing. Bagolini striated lenses are suited to screening for suppression and anomalous retinal correspondence under conditions closest to everyday viewing. The Worth 4-dot test is useful for checking whether suppression is present under moderate binocular dissociation. The synoptophore has stronger binocular dissociation than these tests and is excellent for quantifying the strabismus angle, measuring the fusional range, and making precise judgments of retinal correspondence. The afterimage test has the strongest binocular dissociation and is best for detecting deep anomalous retinal correspondence, but it has high facility requirements. In clinical practice, multiple tests are combined, and the overall picture of binocular vision function is understood by comparing the state close to everyday viewing with the state under the synoptophore.
6. Clinical indications
Section titled “6. Clinical indications”The main clinical indications for synoptophore examination are listed below.
Strabismus assessment
Section titled “Strabismus assessment”- Preoperative evaluation: Quantify the type of strabismus, the strabismus angle (in nine directions), retinal correspondence, and fusional range before surgery. Used for surgical planning and prognosis prediction
- Postoperative evaluation: Quantitatively track postoperative changes in eye position, improvement in fusional range, and recovery of binocular vision function
- Evaluation of paralytic strabismus: Measure objective strabismus angles in nine directions and combine this with the Hess chart to identify the affected muscle
Evaluation of binocular vision function
Section titled “Evaluation of binocular vision function”- Functional evaluation of amblyopia: Quantitatively evaluate binocular vision function before and after amblyopia treatment (presence and degree of simultaneous vision, fusion, and stereopsis)
- Evaluation of fusion function: Quantitatively assess fusion disorders such as convergence insufficiency and divergence insufficiency, and determine whether training is indicated
- Determining indications for strabismus surgery: In cases with established anomalous retinal correspondence, the risk of postoperative diplopia can be assessed in advance
Applications in training
Section titled “Applications in training”- Amblyopia training: Used for amblyopia training with a pleoptocover (penalization)
- Strabismus training: perform training to expand the fusion range and convergence training
- Fusion training: perform repeated training aimed at expanding the fusion range in cases of convergence insufficiency
It has been reported that combining binocular vision training with refractive correction and prism therapy improves eye alignment correction rates and binocular vision in children with esotropia and amblyopia more than either treatment alone4. It has also been shown in amblyopia treatment that the degree of improvement in fusion function correlates with improvement in visual acuity5.
References
Section titled “References”Footnotes
Section titled “Footnotes”-
Fu T, Wang J, Levin M, Su Q, Li D, Li J. Fusional vergence detected by prism bar and synoptophore in chinese childhood intermittent exotropia. J Ophthalmol. 2015;2015:987048. PMID: 25954512. PMCID: PMC4411439. doi:10.1155/2015/987048 ↩
-
Haque S, Toor S, Buckley D. Are Horizontal Fusional Vergences Comparable When Measured Using a Prism Bar and Synoptophore? Br Ir Orthopt J. 2024;20(1):85-93. PMID: 38525409. PMCID: PMC10959145. doi:10.22599/bioj.326 ↩
-
Plaumann MD, Roberts KL, Wei W, Han C, Ooi TL. Refining Clinical Quantification of Depth of Suppression in Amblyopia through Synoptophore Measurement. Life (Basel). 2023;13(9):1900. PMID: 37763304. PMCID: PMC10532546. doi:10.3390/life13091900 ↩
-
Liang J, Pang S, Yan L, Zhu J. Efficacy of binocular vision training and Fresnel press-on prism on children with esotropia and amblyopia. Int Ophthalmol. 2023;43(2):583-588. PMID: 35945412. doi:10.1007/s10792-022-02461-9 ↩
-
Lv Z, Tao Z, Hu G, Deng H. Significance of binocular fusion in enhancing visual acuity during amblyopia treatment. Transl Pediatr. 2024;13(10):1767-1776. PMID: 39524389. PMCID: PMC11543132. doi:10.21037/tp-24-125 ↩