Cranial neuritis is a general term for diseases in which inflammation of the cranial nerves leads to nerve destruction or demyelination. It can affect a single cranial nerve or multiple cranial nerves simultaneously. The latter is called polyneuritis cranialis (PNC).
PNC is considered a rare subtype of Guillain-Barré syndrome (GBS). In the GBS classification proposed by Wakerley et al. in 2014, PNC is defined as presenting only with ocular motor disturbances and bulbar symptoms, without limb weakness or ataxia 1).
A literature review of PNC reported a median age of 40 years in 20 cases, with 75% being male 3). Facial weakness was present in 70%, and normal deep tendon reflexes in 50% 3). When cranial nerves involved in eye movement (III, IV, VI) are affected, diplopia and ophthalmoplegia become the main symptoms.
QWhat is the difference between cranial neuritis and multiple cranial neuritis?
A
Cranial neuritis is a general term for inflammation of the cranial nerves. When a single cranial nerve is affected, it is called cranial neuritis; when multiple cranial nerves are affected simultaneously, it is called multiple cranial neuritis (polyneuritis cranialis). Multiple cranial neuritis is classified as a rare subtype of GBS.
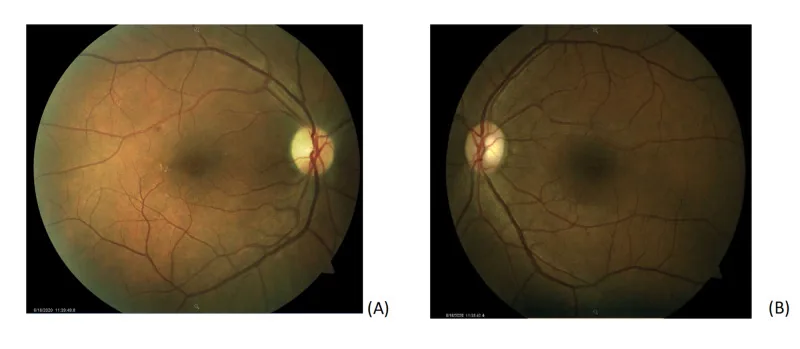
Rho J, et al. A Case of Non-Arteritic Anterior Ischemic Optic Neuropathy with COVID-19. Cureus. 2020. Figure 1. PMCID: PMC7785499. License: CC BY.
Color fundus photographs of both eyes; the right eye (A) shows microaneurysms and exudates along the superotemporal vascular arcade, as well as temporal pallor of the optic disc, while the left eye (B) is normal. This corresponds to optic disc pallor discussed in the section “2. Main symptoms and clinical findings.”
Facial asymmetry/numbness: Causes facial paralysis due to facial nerve (cranial nerve VII) impairment and decreased facial sensation due to trigeminal nerve (cranial nerve V) impairment.
Dysphagia/voice changes: Occur due to impairment of the glossopharyngeal nerve (cranial nerve IX) and vagus nerve (cranial nerve X).
Dizziness/tinnitus: Occur due to impairment of the vestibulocochlear nerve (cranial nerve VIII).
Dysarthria: Occurs due to impairment of the hypoglossal nerve (cranial nerve XII), causing tongue movement disorders.
Headache: Frequently seen as a concomitant symptom of cranial neuritis.
Clinical findings (findings confirmed by physician examination)
Facial nerve palsy (VII): Presents with facial asymmetry, incomplete eye closure, and taste disturbance. Severity is assessed using the House-Brackmann classification 2).
In multiple cranial neuritis, deep tendon reflexes are often decreased or absent 1)3). If meningeal signs are present, it suggests an underlying meningitis.
Among infectious causes, Lyme disease (Borrelia burgdorferi infection) is important. Neuroborreliosis develops in 10–15% of untreated Lyme disease patients and presents with the triad of lymphocytic meningitis, cranial neuritis, and radiculitis 4).
Cranial neuritis after SARS-CoV-2 infection has also been reported. In two cases of multiple cranial neuritis predominantly involving the hypoglossal nerve after severe COVID-19 pneumonia, marked improvement was observed after IVIG administration 1). The mechanism is suggested to be immune-mediated rather than direct neural invasion 1).
In PNC as a subtype of GBS, serum anti-GQ1b IgG antibodies are detected in 47% of cases 3). The most common preceding infection is Mycoplasma pneumoniae 3).
A case of PNC in a 16-year-old after COVID-19 vaccination (BNT162b2) has also been reported 2). However, the risk of vaccine-related neurological complications is much lower than that of COVID-19 infection itself 2).
QIs there a link between COVID-19 and cranial neuritis?
A
Multiple cases of cranial neuritis (especially multiple cranial neuritis) following SARS-CoV-2 infection have been reported 1)5). The pathogenesis is thought to be primarily an immune-mediated reaction after infection rather than direct viral invasion. Cases after COVID-19 vaccination have also been reported, but the risk is lower than that from infection itself 2).
Contrast-enhanced MRI is the most important examination. In cranial neuritis, contrast enhancement of the affected cranial nerve is a characteristic finding. MRI sequences using CISS (constructive interference in steady state) can depict cranial nerves more clearly.
Key points for MRI acquisition are as follows:
T1-weighted and T2-weighted images as the basis
Inflammatory diseases combine FLAIR and STIR sequences
Optic neuritis benefits from coronal fat-suppressed contrast-enhanced T1-weighted images
For evaluation of demyelinating lesions, whole-brain axial FLAIR is important
If a vascular etiology is suspected, CTA, MRA, or catheter angiography should be added. CT is useful as an emergency screening tool.
In nerve conduction studies, loss of F-waves is an important early sign of proximal demyelination2). Blink reflex testing evaluates abnormalities in R1 and R2 responses3).
Measurement of anti-ganglioside antibodies (anti-GM1, anti-GQ1b, anti-GD1a, etc.) is useful for diagnosing GBS subtypes3). However, a negative antibody test does not rule out PNC.
As part of the search for infectious causes, serological tests for Lyme disease, syphilis, anti-AQP4 antibodies, and anti-MOG antibodies are performed as appropriate.
Steroid pulse therapy: Intravenous methylprednisolone 1,000 mg/day for 3 days. Particularly effective when accompanied by optic neuritis.
After steroid pulse therapy, oral prednisolone is started at 0.5 mg/kg/day and tapered by 5–10 mg every 3–4 days.
Oral steroid monotherapy is not performed because it increases the risk of recurrence of optic neuritis.
Before systemic steroid administration, it is essential to rule out infections such as hepatitis B.
QCan recovery be expected with treatment for cranial neuritis?
A
Identification of the underlying cause and appropriate treatment can lead to improvement of neurological symptoms in many cases. In the GBS subtype PNC, many reports show marked improvement after IVIG administration 1)3). However, in cases with visual impairment, recovery of visual function may be incomplete 3).
Demyelination is the destruction of the myelin sheath surrounding the axon of myelinated nerves. When the myelin sheath is destroyed, saltatory conduction becomes impossible, leading to nerve conduction impairment. In the GBS subtype PNC, the demyelinating type is predominant, and electrophysiologically, loss of F-waves, conduction block, and prolonged distal latency are observed 2)5). On the other hand, the axonal type is characterized by reduced amplitude of compound muscle action potentials 5).
In post-infectious cranial neuritis, molecular mimicry is an important pathology. Due to structural similarity between glycolipids carried by the preceding infectious pathogen and gangliosides present in the myelin sheath of cranial nerves, cross-reactive autoantibodies are produced 3).
The main anti-ganglioside antibodies detected in PNC are anti-GQ1b IgG (47%), followed by anti-GT1a and anti-GD1a IgG antibodies 3). These antibodies target the myelin sheath of cranial nerves and trigger complement-mediated demyelination.
The mechanism of cranial neuritis after COVID-19 is not fully understood.
De Gennaro et al. (2021) reported two cases of multiple cranial neuritis after severe COVID-19 pneumonia. In both cases, neurological symptoms appeared about one month after infection, and SARS-CoV-2 PCR tests had become negative. Since marked improvement was observed after IVIG administration, they concluded that post-infectious immune-mediated mechanisms, rather than direct neural invasion, were the main cause 1).
Candidate mechanisms are as follows 1).
Neural invasion via ACE2 receptor: The spike protein of SARS-CoV-2 may bind to ACE2 receptors expressed in the CNS and PNS, allowing retrograde entry from nerve terminals.
Immune-mediated reaction: A delayed abnormal immune response similar to GBS and MFS occurs.
Cytokine cascade: Elevated IL-8 in cerebrospinal fluid has been reported, suggesting involvement of inflammatory cytokines5).
QWhy are cranial nerves damaged after infection?
A
Molecular mimicry is considered the main mechanism in post-infectious cranial neuritis. Structural similarity between pathogen glycolipids and gangliosides of the cranial nerve myelin leads to production of cross-reactive autoantibodies, triggering demyelination of cranial nerves3). The good response to IVIG also supports this immune-mediated mechanism1).
7. Latest Research and Future Perspectives (Research-stage Reports)
Manganotti et al. (2021) reported GBS/PNC complications in 5 COVID-19 patients. Four received IVIG (0.4 g/kg for 5 days) with improvement in neurological symptoms. Elevated CSF IL-8 was found in 3 cases, suggesting immune-mediated peripheral neuropathy associated with SARS-CoV-2 infection5).
Kulsirichawaroj et al. (2022) reported a case of a 16-year-old Thai woman who developed PNC 3 hours after the first dose of BNT162b2 mRNA vaccine. She presented with right-sided cranial nerve V, VII, IX, and X deficits, with absent F-waves and contrast enhancement of the right facial nerve. After IVIG, all symptoms except facial palsy recovered within 4 weeks2).
Li et al. (2023) reported a rare case of a 54-year-old man with PNC complicated by visual impairment. Serum anti-GM1 and anti-GD1a IgG antibodies were positive, and rapid neurological improvement occurred after IVIG. Visual recovery required additional steroid therapy, but complete recovery to 6/6 vision in both eyes was achieved after one month3). In a literature review of 32 cases of GBS combined with optic neuritis, poor visual prognosis was 47%, while neurological prognosis was generally favorable.
De Gennaro R, Gastaldo E, Tamborino C, Baraldo M, Casula N, Pedrali M, et al. Selective cranial multineuritis in severe COVID-19 pneumonia: two cases and literature review. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2021;42(5):1643-1648. doi:10.1007/s10072-021-05087-4. PMID:33515336; PMCID:PMC7847241.
Kulsirichawaroj P, Sanmaneechai O, Wittawatmongkol O, et al. Polyneuritis cranialis associated with BNT162b2 mRNA COVID-19 vaccine in a healthy adolescent. Vaccines. 2022;10(1):134. doi:10.3390/vaccines10010134.
Hui Li, Zhijun Li, Bo Huang, Na Tang, Shabei Xu, Wenhao Zhu. Co-occurrence of polyneuritis crainials and visual impairment: a case report and literature review. Neurol Sci. 2022;44(5):1563-1574. doi:10.1007/s10072-022-06580-0.
Omotosho YB, Sherchan R, Ying GW, Shayuk M. A Unique Case of Bannwarth Syndrome in Early Disseminated Lyme Disease. Cureus. 2021;13(4):e14680. doi:10.7759/cureus.14680. PMID:33912367; PMCID:PMC8071476.
Manganotti P, Bellavita G, D’Acunto L, Tommasini V, Fabris M, Sartori A, et al. Clinical neurophysiology and cerebrospinal liquor analysis to detect Guillain-Barré syndrome and polyneuritis cranialis in COVID-19 patients: A case series. Journal of medical virology. 2021;93(2):766-774. doi:10.1002/jmv.26289. PMID:32662899; PMCID:PMC7405169.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.