Punctal cauterization is a permanent punctal occlusion method that uses thermocautery or electrocautery to surgically close the punctum and the vertical canaliculus. By closing the punctum, tear drainage is blocked, increasing the volume and retention time of tears on the ocular surface, thereby treating ocular surface diseases.
Punctal cauterization was first reported by Beetham in 1934. In 1978, Dohlman reported punctal closure using diathermy for keratoconjunctivitis sicca, and the technique has since been refined with modern cautery devices.
Punctal occlusion methods include punctal cauterization, dissolvable punctal inserts, silicone punctal plugs, argon laser photocoagulation, and surgical punctal/canalicular closure. Currently, plug occlusion is the most common, but for severe cases with repeated plug loss, punctal cauterization is a useful option 2).
QWhat is the difference between punctal cauterization and punctal plugs?
A
Punctal plugs are small silicone or collagen pieces inserted into the punctum for temporary to semi-permanent closure, allowing removal or replacement. In contrast, punctal cauterization permanently closes the punctum by cautery and is generally irreversible. Punctal cauterization is chosen for patients who cannot retain plugs or cannot tolerate them.
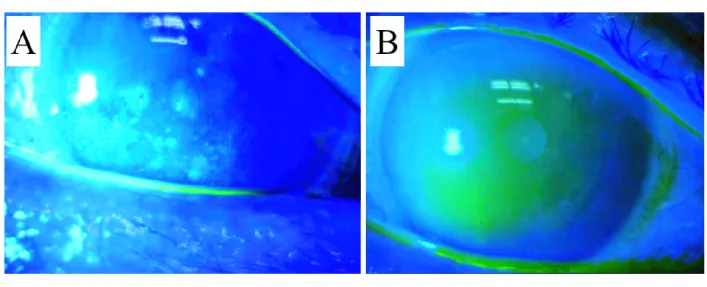
Kuroda K, Toshida H, Sorita Y, et al. Surgical Punctal Occlusion; Combined Lacrimal Canaliculi Cauterization and Punctal Suturing for Severe Dry Eye. Journal of Ophthalmic & Vision Research. 2023 Apr 19; 18(143):$2. Figure 3. PMCID: PMC10172797. License: CC BY.
Fluorescein staining shows improvement of punctate epithelial keratopathy after surgery, comparing before and after. This image illustrates how improved tear retention is reflected in corneal epithelial findings.
Punctal cautery is used for ocular surface diseases associated with aqueous-deficient dry eye.
Sjögren’s syndrome (SS): Severe cases with markedly reduced tear secretion where eye drops cannot maintain adequate moisture are candidates for punctal occlusion.
Punctal cautery can be performed in an outpatient setting. The upper and lower puncta can be treated in a single session, or one punctum at a time to adjust the effect.
Topical anesthesia: Instill proparacaine or tetracaine. Apply lidocaine jelly directly to the punctum.
Disinfection: Wash the eyelid and eye with povidone-iodine solution.
Local injection anesthesia: Inject 1–2% lidocaine without epinephrine subcutaneously around the inner canthus and punctum, then wait about 5 minutes.
Cautery: Insert the tip of a disposable handheld low-temperature cautery device into the punctum and vertical canaliculus, then gradually withdraw while applying short pulsed cautery. The entire process usually finishes within 15–20 seconds.
Endpoint: Whitening and shrinkage of the punctum are the endpoints of cautery.
Post-procedure: Apply antibiotic ointment (e.g., erythromycin) and instruct the patient to continue for one week.
Avoid excessive cautery of the canaliculus or punctum. There is a risk that the tip may become entangled in the cauterized tissue, causing tissue damage.
Disposable thermal cautery: A high-temperature tip is inserted directly into the punctum and canaliculus. Reports using OPTEMP II V (590–690°C) show a recanalization rate as low as 0–1.4%1).
Monopolar radiofrequency cautery: Uses an electrosurgical unit in the operating room. The recanalization rate is reported as 9.7%1).
Surgical closure methods
Canalicular cauterization + suture closure: Remove the canalicular epithelium with a diamond burr or cautery, then close with 6-0 Vicryl. Recanalization rate 5–8%1).
Tissue plug method: Fill the cauterized canaliculus with fibrous tissue harvested from the caruncle. Recanalization rate 8%1).
Punctal switch graft: Rotate the eyelid margin epithelium adjacent to the punctum 180° to cover the punctum. Recanalization rate 9%1).
In a systematic review by Ranjan et al. (9 studies, 150 patients), the method of directly inserting a disposable thermal cautery tip into the punctum showed a lower recanalization rate than monopolar high-frequency cautery1).
Punctal cauterization improves both subjective symptoms and objective measures of dry eye1)2).
Outcomes of thermal cautery and surgical closure methods are shown below.
Measure
Thermal cautery
Surgical closure
Schirmer improvement
+2.5 mm
+2.1 mm
TBUT improvement
+0.8 seconds
+0.6 seconds
Recanalization rate
0–38.7%
5–9%
No statistically significant differences were observed between the two techniques in Schirmer test values (P=0.17), TBUT (P=0.18), or recanalization rate (P=0.22)1).
According to the TFOS DEWS III report, a retrospective study of 80 patients who underwent punctal cautery found that 54% reported significant improvement in subjective symptoms, and 19% had reduced corneal staining severity. The overall recanalization rate was 21%, and the use of steroid eye drops increased the recanalization rate (30% vs 15%, P=0.0003)2).
In a study of 65 patients with cicatricial disease, the recanalization rate after punctal cautery was only 11%, suggesting that fibrosis associated with the underlying disease may have contributed to maintaining closure2).
QCan punctal cautery be reversed?
A
Punctal cautery is generally a permanent and irreversible procedure. However, recanalization (reopening of the cauterized punctum) occurs in 0–38.7% of cases. If epiphora becomes a problem, clinical recanalization of the punctum does not necessarily mean normal tear drainage.
Punctal cautery is generally well tolerated by patients and has few complications.
Transient pain and swelling: May occur after the procedure. Usually resolves spontaneously.
Epiphora (tearing): A common complication of all punctal closure methods. Can be prevented by appropriate patient selection through temporary punctal occlusion.
Granuloma: May form on exposed sclera or at the cautery site. Reported incidence is 1.7% 1).
In a systematic review by Ranjan et al., all 9 studies on punctal cautery were single-arm trials (no control group), and meta-analysis was not feasible. The absence of randomized controlled trials (RCTs) is the major challenge, and they concluded that RCTs are necessary to confirm the true efficacy of punctal cautery 1).
Comparison with punctal plugs: Direct comparison of recanalization rates and efficacy between permanent punctal plugs and cautery.
Comparison among cautery devices: Elucidation of differences in recanalization rates among disposable thermal cautery, radiofrequency monopolar cautery, and surgical closure methods 1).
Effect of postoperative anti-inflammatory drugs: It has been suggested that steroid eye drops may increase the recanalization rate, and comparison with cyclosporine eye drops is being considered2)
Outcome analysis by disease: Differences in treatment response according to the etiology of ADDE (SS, GVHD, SJS, etc.)
QCan tearing occur after punctal cauterization?
A
Tearing is a common complication of all punctal occlusion methods, but if it is confirmed preoperatively that tearing does not occur with temporary occlusion using dissolvable punctal plugs, the likelihood of tearing after cauterization is low. The risk is even lower in patients with severely reduced tear secretion.
Ranjan A, Basu S, Singh S. Punctal cautery in dry eye disease: A systematic review. The ocular surface. 2024;34:235-240. doi:10.1016/j.jtos.2024.08.006. PMID:39127391; PMCID:PMC7617785.
Jones L, Craig JP, Markoulli M, Karpecki P, Akpek EK, Basu S, Bitton E, Chen W, et al. TFOS DEWS III: Management and Therapy. American journal of ophthalmology. 2025;279:289-386. doi:10.1016/j.ajo.2025.05.039. PMID:40467022.
Wang Y, Carreno-Galeano JT, Singh RB, Dana R, Yin J. Long-term Outcomes of Punctal Cauterization in the Management of Ocular Surface Diseases. Cornea. 2021;40(2):168-171. PMID: 32467449.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.