Loiasis is an infectious disease caused by the filarial nematode Loa loa, which parasitizes the subcutaneous and submucosal tissues of humans. Because adult worms migrating under the bulbar conjunctiva can be seen with the naked eye, it is also called “African eye worm.”
Loa loa infects only humans and primates1). Males are about 3 cm long, females 5–7 cm, with a diameter of 0.4–0.5 mm1). Adult worms can survive for more than 20 years, and mature females produce 12,000–39,000 microfilariae per day.
The vector is the blood-sucking deerfly of the genus Chrysops. Its habitat is forested and swampy areas of West and Central Equatorial Africa1), with endemic countries including Angola, Cameroon, Central African Republic, Congo, Gabon, Nigeria, and others. Over 10 million people are infected, and more than 14 million live in high-risk areas.
Traditionally considered a benign disease, recent reports indicate that the population-attributable risk fraction of death associated with microfilaraemia is 14.5%, questioning its benign nature.
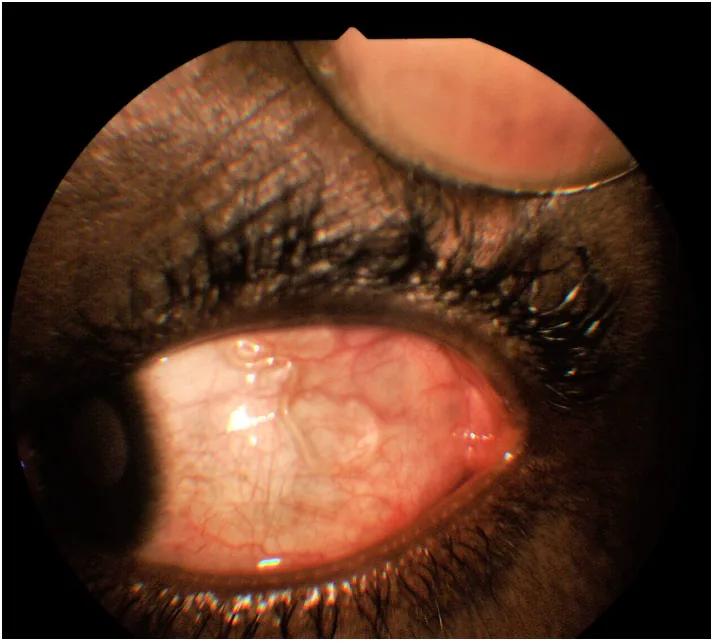
Ogugua Ndubuisi Okonkwo, Adekunle Olubola Hassan, Taofik Alarape, Toyin Akanbi, et al. Removal of adult subconjunctival Loa loa amongst urban dwellers in Nigeria 2018 Nov 14 PLoS Negl Trop Dis. 2018 Nov 14; 12(11):e0006920 Figure 5. PMCID: PMC6261630. License: CC BY.
A translucent worm is seen traversing under the prominent blood vessels of the bulbar conjunctiva. This shows the appearance of Loa loa migrating just beneath the conjunctival surface.
In long-term residents of endemic areas, many infections are asymptomatic. In contrast, travelers and short-term visitors often develop a “hyperreactive syndrome” with marked eosinophilia, angioedema, generalized pruritus, and elevated IgE. Ocular symptoms commonly include foreign body sensation and discomfort. If the worm invades the eye, pain and photophobia may occur.
Subconjunctival worm migration: The adult worm migrating under the bulbar conjunctiva can be seen with the naked eye. This is a pathognomonic sign of the disease. It usually does not cause permanent tissue damage.
Eyelid edema: Edema occurs due to migration of the adult worm around the eye.
Intraocular filariasis (rare): The worm invades the anterior chamber or vitreous cavity. Findings include fibrinous membrane formation, anterior chamber cells/flare, and keratic precipitates. Visual acuity may decrease from 6/24 to light perception.
Systemic Findings
Calabar swelling: Occurs in 50% of patients1). It is a non-erythematous subcutaneous edema, 5–20 cm in size, commonly on the limbs, and resolves spontaneously within hours to 2–4 days1). It is due to a hypersensitivity reaction to the migrating adult worm.
Eosinophilia: Marked peripheral blood eosinophilia is present1).
If you see a worm migrating under the conjunctiva, see an ophthalmologist promptly as it may disappear quickly. The subconjunctival worm can usually be removed by making a small conjunctival incision under local anesthesia. However, since microfilariae remain in the body, systemic treatment with antiparasitic drugs is necessary after worm removal.
Loiasis is caused by infection with Loa loa, transmitted by female deer flies of the genus Chrysops1). These flies are most active between 10 a.m. and 2 p.m., showing a diurnal pattern. Their habitat includes forests and swamps, with peak activity during the rainy season 1).
Transmission route:
Third-stage larvae (L3) enter through the skin when the fly bites
Larvae reach the dermis and mature into adults over 150–170 days
The incubation period is 3–15 months, but can extend up to 3–4 years 1)
Daytime appearance of microfilariae: Microfilariae are sheathed and exhibit diurnal periodicity, peaking at noon 1). This periodicity coincides with the activity time of deer flies.
Risk factors:
Travel to endemic areas (risk increases with exposure over 1 month)
Activities in forests or swampy areas
Symptoms are more pronounced in short-term travelers than in long-term residents
QCan travelers also get infected?
A
Yes, travelers to endemic areas can also get infected. The risk increases especially with stays longer than one month. Travelers tend to have more severe symptoms compared to residents of endemic areas and are more likely to develop “hypersensitivity syndrome” characterized by marked eosinophilia, angioedema, and generalized pruritus.
Definitive diagnosis is based on identification of microfilariae or direct confirmation of adult worms.
Definitive diagnostic methods:
Direct observation and removal of the worm under the conjunctiva for species identification
Detection of microfilariae in blood smear (blood drawn at noon, due to diurnal periodicity) 1)
The detection rate of microfilariae is not always high. It is often negative in people from non-endemic areas 1). Since microfilariae are released into peripheral blood irregularly, multiple blood draws on different days may be necessary 1).
Serological and molecular biological tests:
LISXP-1 IgG4 recombinant antigen test: high specificity
LAMP (loop-mediated isothermal amplification): high sensitivity, also useful for identifying individuals at risk of drug side effects
ELISA antibody test: low specificity, cross-reactivity with other filarial worms
Co-infection with Onchocerca volvulus is clinically important. Because it directly affects treatment selection, differentiation using tests specific to Loa loa is essential.
Drug therapy is the basic treatment for loiasis; surgical removal of the worm alone cannot eradicate systemic microfilariae.
Drug Therapy
Diethylcarbamazine (DEC): First-line drug. Administered at 8–10 mg/kg three times daily for 3 weeks. Effective against both adult worms and microfilariae. Can also be used for prophylaxis. Contraindicated when microfilarial count ≥2,500 mf/mL due to risk of encephalopathy.
Albendazole: Used as pretreatment for high microfilarial loads. Targets adult worms and slowly reduces blood microfilariae. Fewer side effects compared to DEC.
Ivermectin: A single dose reduces microfilariae for over a year but has no activity against adult worms. Risk of encephalopathy in patients with high parasite loads. Case reports have reported cure with ivermectin 200 μg/kg/week for 3 weeks plus albendazole 800 mg/day for 1 month1).
Surgical Treatment
Subconjunctival worm removal: Grasp the worm with forceps when it appears, anesthetize and paralyze with subconjunctival injection of lidocaine containing epinephrine, then remove through a conjunctival incision of 5 mm or less.
Anterior chamber irrigation: Perform anterior chamber irrigation for intraocular filarial worms, followed by subconjunctival injection of steroids and antibiotics. If a fibrinous membrane is present, excision is necessary.
Vitrectomy: Performed for filarial worms in the vitreous body, but this is an extremely rare indication.
QAre the side effects of the medication safe?
A
The main concern with treatment drugs is encephalopathy and retinal hemorrhage caused by rapid killing of blood microfilariae. In patients with low microfilarial load (<2,500 mf/mL), DEC is considered relatively safe. For high-load cases, pretreatment with albendazole is given before switching to DEC or ivermectin. In case reports, patients with negative microfilariae were treated with ivermectin plus albendazole and cured without side effects other than mild pruritus1).
The life cycle of Loa loa is completed between the deerfly (Chrysops) and the human host.
Infection cycle:
Third-stage larvae (L3) enter the skin during the bite of an infected deerfly
Larvae reach the dermis and mature into adults over 150–170 days
Adult worms reside in the dermis and move actively1)
Mature females produce microfilariae in the connective tissue
Microfilariae migrate to peripheral blood, showing diurnal periodicity with a peak at noon1)
Deerflies ingest microfilariae during blood feeding, which develop to L3 inside the fly and infect the next host
Mechanism of Calabar swelling: As adult worms migrate subcutaneously, the host immune system reacts, causing an IgE-mediated hypersensitivity reaction. This presents as transient local edema that resolves spontaneously within hours to days1).
Mechanism of ocular lesions: Adult worms migrate through periorbital tissues to the subconjunctival space1). Subconjunctival migration usually does not cause permanent tissue damage. However, if the worm enters the anterior chamber or vitreous, a strong inflammatory reaction (fibrin membrane formation, uveitis) can lead to vision loss.
Microfilaremia and organ damage: It is hypothesized that obstructive and inflammatory processes of microfilariae in the circulatory system cause retinal vascular lesions (loiasis retinopathy) and other organ damage. This mechanism has been proposed as a hypothesis to explain the increased risk of death (population attributable fraction 14.5%).
Research on loiasis is mainly progressing toward improving diagnostic methods and establishing safe treatment strategies.
Development of new diagnostic methods: An immunochromatographic test using the LISXP-1 antigen has been developed, achieving 94% sensitivity and 100% specificity compared to the control group. The LAMP method is highly sensitive and also useful for identifying individuals at risk of adverse reactions after ivermectin treatment. These tests may contribute to improving the safety of mass drug administration programs in endemic areas.
Challenges in mass drug administration: Ivermectin mass drug administration programs for onchocerciasis are limited in areas co-endemic with loiasis due to the risk of severe adverse reactions. Rapid assessment methods for microfilarial density are being developed, and safe mass drug administration is expected to be realized.
Lunardon L, Romagnuolo M, Cusini M, Veraldi S. A Case of Possible Loiasis Contracted in Cameroon and Diagnosed in Milan, Italy, and Review of Cases Published in Dermatological Journals. Case reports in dermatology. 2021;13(2):389-393. doi:10.1159/000513939. PMID:34413738; PMCID:PMC8339440.
Hasnaoui I, Hazil Z, Krichen MA, Hassina S, Akkenour Y, Serghini L, et al. [Ocular Loa loa filariasis]. J Fr Ophtalmol. 2024;47(4):104124. PMID: 38452599.
VAN BOGAERT L, DUBOIS A, JANSSENS PG, RADERMECKER J, TVERDY G, WANSON M. Encephalitis in loa-loa filariasis. J Neurol Neurosurg Psychiatry. 1955;18(2):103-19. PMID: 14381919.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.