Cyclopia, also called synophthalmia or cyclocephaly, is the most severe facial manifestation of holoprosencephaly (HPE). It involves the fusion of both eyes into a single median orbit in the center of the face.
HPE is a congenital anomaly in which the forebrain fails to divide properly into left and right hemispheres, and it is classified into four subtypes 1).
Subtype
Characteristics
Alobar (most severe)
Complete failure of forebrain division
Semilobar
Partial separation
Lobar type (mildest)
Continuity of frontal cortex preserved
Interhemispheric variant
Incomplete separation of posterior parietal region
Cyclopia is the most extreme manifestation of alobar HPE, accounting for 10–18% of all HPE cases 4). Its incidence is 1 per 100,000 births, with a 58% female predominance. The higher rate of stillbirth in males is considered a contributing factor to the female predominance.
The degree of facial dysmorphism correlates with the severity of brain abnormalities 1). In mild HPE, findings are limited to microcephaly, microphthalmia, and hypotelorism, whereas severe cases involve cyclopia, proboscis, and median facial cleft.
Cyclopia is a lethal anomaly incompatible with life, and most cases result in miscarriage or stillbirth. The longest recorded survival is 1 day.
The cyclops (one-eyed giant) of ancient Greek mythology, known as Polyphemus in Homer’s Odyssey from the 8th-7th century BCE, is thought to have possibly been inspired by actual infants with cyclopia.
QCan a baby with cyclopia survive?
A
It is a lethal abnormality incompatible with life. Most cases result in intrauterine death or stillbirth, and even if born, death occurs within hours. The longest recorded survival is one day.
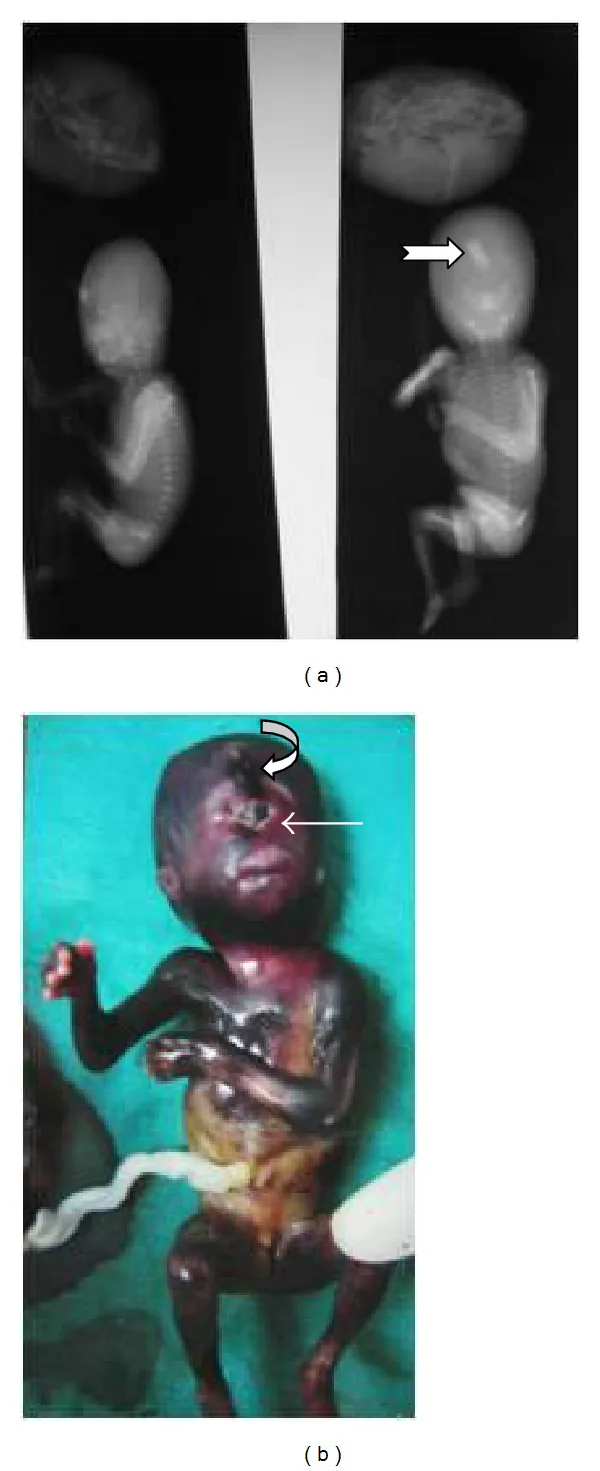
Raman R, Mukunda Jagadesh G. Antenatal Diagnosis of Alobar Holoprosencephaly. Case Rep Radiol. 2014 Jul 14;2014:724671. Figure 3. PMCID: PMC4122072. License: CC BY.
B is a specimen photograph showing a single central orbit and a proboscis above it. Together with the X-ray image in A, it demonstrates severe midline facial dysplasia and absence of nasal structures.
Taifour et al. (2025) reported a 2000g female infant who was stillborn at 30 weeks of preterm delivery. The infant had a single median fused eye and a proboscis, no cleft lip or palate, but had edema of the neck and shoulders, scaly skin, and polydactyly with six fingers on each hand. Ultrasound revealed ventriculomegaly, intracranial calcifications, thalamic fusion, absent septum pellucidum, and agenesis of the corpus callosum 1).
Kunwar et al. (2021) reported a 1.25kg female infant who died in utero at 31 weeks from a 40-year-old woman with chronic alcohol use (G6P5+1). The infant had a single eye and a proboscis, with the nose absent in its normal position 2).
Matalliotakis et al. (2021) reported a case of a 27-year-old woman after IVF, in whom a single central orbital cavity was identified on 3D ultrasound at 22 weeks. The 350g female infant exhibited cyclopia (fused two eyes) with fused eyelids, a small proboscis, and displacement of the left ear. Parental karyotype testing showed no abnormalities 3).
Nik Lah et al. (2023) reported a case of dichorionic diamniotic twins in a 36-year-old woman (G9P4+4) with consanguineous marriage. The first child (1.46 kg) had true cyclopia, and the second child (1.68 kg) had synophthalmia; both infants had a proboscis. Apgar scores were 3 at 1 minute and 2 at 10 minutes, and they died approximately 25 minutes after birth 4).
The etiology of cyclopia is multifactorial, involving genetic and environmental factors. Since 18–25% of infants with HPE have a single-gene syndrome and 24–45% have chromosomal abnormalities (most commonly trisomies 13, 18, and 21), genetic and chromosomal testing is recommended 1).
Female predominance: 58% of cases occur in females
Multiple pregnancy: Risk is increased especially in twin pregnancies
Syndromic associations: Smith-Lemli-Opitz syndrome, etc.
Maternal Factors
Infections: TORCH infections, toxoplasmosis
Drug exposure: Retinoic acid, antiepileptic drugs, lithium
Lifestyle: Alcohol, smoking
Metabolic disorders: Gestational diabetes
Plant toxins: Cyclopamine (an alkaloid from corn lily)
Individual case reports have identified the following risk factors.
Toxoplasma infection: There have been cases with a history of first contact with cats and findings associated with congenital toxoplasmosis (ventriculomegaly, intracranial nodules, placental hypertrophy, hyperechoic bowel)1).
Chronic alcohol use: Stillbirth of a cyclops infant has been reported in a 40-year-old chronic alcohol user2).
IVF procedure: There are reports of cyclopia occurring in pregnancies following in vitro fertilization3).
Consanguineous marriage: A first-degree consanguineous couple had a history of four miscarriages and a previous child with Patau syndrome who died4).
Pericentric inversion of chromosome 9: inv(9)(p11,q13) is considered a normal variant in the general population, but an association with congenital anomalies has also been reported4).
QCan cyclopia be prevented during pregnancy?
A
No specific preventive measures have been established. However, management of gestational diabetes, avoidance of alcohol, retinoic acid, and antiepileptic drugs, and prevention of TORCH infections are recommended. Regular prenatal checkups enable early detection.
Gross and pathological evaluation: Confirmation of external malformations and anatomical examination1).
Chromosomal analysis: Parental karyotyping and amniocentesis are recommended3)4).
TORCH testing: Evaluates involvement of infectious diseases1)3).
QCan prenatal ultrasound detect cyclopia early?
A
NT scan at 11–14 weeks of pregnancy may detect features of HPE. Diagnosis is usually confirmed by anomaly scan after 20 weeks. 3D ultrasound can accurately assess facial abnormalities.
Discussion of pregnancy termination options: In severe cases, after diagnosis is confirmed, pregnancy termination should be discussed with the family 1).
If pregnancy is continued: Consultations with pediatric neurology, neurosurgery, and neonatology should be arranged 1).
Determination of delivery mode: Based on the presence or absence of extracranial abnormalities and other factors. It is determined using the same criteria as for normal delivery1).
Supportive care: Aggressive resuscitation is considered unlikely to contribute to the infant’s survival4). In the twin case reported by Nik Lah et al., aggressive resuscitation was not performed due to conditions incompatible with life support4).
Ophthalmic management: In trisomy 13, ophthalmic treatment is rarely actively performed due to poor life prognosis, but in recent years, life prognosis has been improving with neonatal intensive care.
Between the 18th and 28th day of gestation, the forebrain divides into left and right halves. During neural tube formation, the neural plate folds to form the neural tube, and its anterior part differentiates into three primary brain vesicles: the forebrain, midbrain, and hindbrain.
The forebrain further differentiates into the telencephalon (cerebrum) and the diencephalon (thalamus and hypothalamus). The optic vesicles develop from the diencephalon. Around day 22, two grooves appear on each side of the developing forebrain and protrude as optic vesicles. The optic vesicles grow laterally and, upon approaching the surface ectoderm, secrete BMP4 to induce the lens placode. This reaction requires expression of the PAX6 gene.
Abnormal differentiation theory of the prechordal mesoderm: Irregular growth of the frontonasal process leads to absence of the nose, labial arch, ethmoid bone, and premaxilla, causing the eye to be displaced to the midline 3).
Arterial circulation theory: Midline fusion of the aortic arch plexus creates mechanical traction on the optic primordia, resulting in midline fusion 3).
Incomplete division of the lens primordium: Two sets of lens fibers persist, leading to fusion into a single eye 4).
In cases with normal chromosomes, the risk is 6%; in those with abnormal karyotypes, it is 1%. For autosomal dominant inheritance, the risk is as high as 50%, and for recessive inheritance, 25%. Genetic counseling for the next pregnancy is important.
Taifour W, Ranjous Y, Khoury M, Alshammy H, Abbassi H. Cyclopia Syndrome with Neck Presentation: A Case of Alobar Holoprosencephaly and Prenatal Diagnostic Challenges. Int Med Case Rep J. 2025;18:893-898.
Kunwar A, Shrestha BM, Shrestha S, Paudyal P, Rawal S. Cyclopia with proboscis: A rare congenital anomaly. Clin Case Rep. 2021;9:e04466.
Matalliotakis M, Trivli A, Matalliotaki C, Moschovakis A, Hatzidaki E. Cyclopia: The Face Predicts the Future. Cureus. 2021;13(8):e17114.
Nik Lah NA, Taib F, Mohamad Zon E, Engku Ismail EH, Annuar AA. Pericentric Inversion of Chromosome 9 in Twins With Cyclopia: A Rare Entity. Cureus. 2023;15(2):e34562.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.