The uveoscleral outflow pathway was discovered by Anders Bill in 1965 through animal experiments. It is a route by which aqueous humor flows across the ciliary body and iris root into the suprachoroidal space. Prostaglandin analogs lower intraocular pressure by increasing outflow through this pathway.
In 1905, Heine reported the surgical creation of a cyclodialysis cleft for refractory glaucoma, but it did not become widely adopted due to postoperative hypotony and acute intraocular pressure elevation after cleft closure. Advances in device design and biocompatibility have led to the development of new devices aiming for controlled, sustained aqueous outflow.
In the classification of MIGS, suprachoroidal procedures are positioned as an independent category alongside trabecular surgery and subconjunctival filtering devices1)3).
A general term for MIGS devices targeting the uveoscleral outflow pathway. They connect the anterior chamber to the suprachoroidal space, increasing aqueous humor outflow via an alternative pathway to lower intraocular pressure. Unlike trabecular bypass stents (iStent, Hydrus) that target the main pathway, suprachoroidal devices utilize the alternative pathway 4). There are two types: extraocular approach (GMS, STARflo) and intraocular approach (CyPass, MINIject), each with different surgical invasiveness and intraocular pressure-lowering effects 1).
The extraocular approach accesses the suprachoroidal space via a transscleral incision. It requires manipulation of the conjunctiva and sclera, which may complicate future filtration surgery. However, it allows for more extensive tissue dissection and is expected to achieve greater intraocular pressure reduction compared to the intraocular approach.
Gold Micro Shunt (GMS)
Material: Medical-grade 24K gold. Based on the finding that gold is well tolerated intraocularly.
Structure: Two rectangular fused leaflets. Proximal end has 60 holes of 100 μm and 1 hole of 300 μm; distal end has a grid of 117 holes of 110 μm.
Procedure: Fornix-based conjunctival flap → Full-thickness scleral incision 2–3 mm posterior to the limbus → Exposure of suprachoroidal space → Creation of an intracameral tunnel → Device insertion.
Modified GMS+: Relocation of fins and design change from channel to post to enlarge the outflow area.
STARflo
Material: STAR Biomaterial (porous medical-grade silicone). Designed to promote tissue integration and inhibit fibrosis.
Structure: Three-part integrated design: head, neck, and body.
Procedure: Conjunctival flap → partial-thickness scleral flap → insert the head into the anterior chamber → full-thickness scleral incision at the posterior edge of the flap → insert the body into the suprachoroidal space
The ab interno approach uses a clear corneal incision and intraoperative gonioscopy. Since the conjunctiva and sclera are preserved, there is less impact on future filtration surgery.
CyPass Micro-Stent
Material: Polyimide. Length 6.35 mm, outer diameter 0.5 mm, inner diameter 300 μm
Structure: Fenestrations along the entire length. Promotes outflow
Procedure: Clear corneal incision → deepen anterior chamber with viscoelastic → visualize with intraoperative gonioscopy → create a micro-cyclodialysis by blunt dissection from the scleral spur → insert the stent
Current status: Voluntarily withdrawn from the market in 2018 due to corneal endothelial cell loss2)3)
MINIject
Developer: iSTAR Medical (Belgium)
Classification: Listed in the EGS guidelines as a suprachoroidal MIGS1)
Features: Positioned as the only ab interno suprachoroidal MIGS device after the withdrawal of CyPass
Approach: Ab interno. Designed to reduce impact on corneal endothelium
Unlike conventional devices, this is a new technique that utilizes endogenous cyclodialysis as a filtration pathway into the uveoscleral outflow tract. An allograft is placed in the cleft to prevent re-occlusion. Using the CycloPen™, an intraocular approach creates a cyclodialysis (1–2 clock hours), and a micro-trephined allograft (5 mm long × 500 μm wide) is fully placed into the cleft. Since it does not protrude into the anterior chamber, it avoids effects on the corneal endothelium.
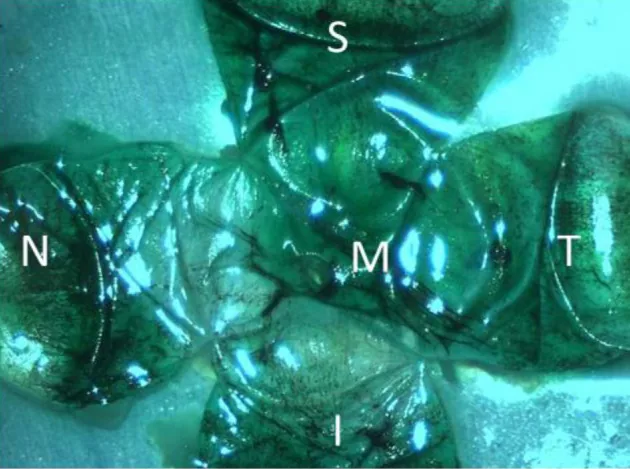
Buckman PN, Brinker BA, Kapeller LE, et al. Validation of the EYEMATE-SC Suprachoroidal Pressure Transducer for Telemetric Measurement of Intraocular Pressure in Normal Ex Vivo Canine and Equine Globes: Preliminary Results. Vet Ophthalmol. 2025. Figure 2. PMID: 40883863; PMCID: PMC12488533. DOI: 10.1111/vop.70071. License: CC BY 4.0.
Intraoperative photograph showing manipulation of a suprachoroidal device. It illustrates the positional relationship as the device tip is advanced from the scleral incision into the suprachoroidal space.
GMS: A three-group RCT by Skaat et al. compared two types of GMS (internal channel 24 μm or 48 μm) with the Ahmed glaucoma valve. The cumulative success rates at 5 years were 77.8% in the Ahmed group, 77.8% in the 24 μm GMS group, and 72.7% in the 48 μm GMS group. In contrast, a retrospective study of the second-generation GMS+ by Hueber et al. reported a 97% failure rate at 4 years, with 77% requiring secondary surgery.
STARflo: Initial clinical trials reported a reduction in intraocular pressure from 37.0 to 14.5 mmHg at 12 months, but a European prospective study found that 45% required additional surgery at 24 months, with corneal endothelial cell loss and corneal degeneration (12.5%) observed.
In GMS studies, a report on 55 eyes with refractory glaucoma showed a 2-year limited success rate of 67.3% and complete success rate of 5.5%. The cause of failure in 66.6% of cases was inflow obstruction due to inflammatory membrane formation at the anterior tip of the shunt.
The CyPass Micro-Stent showed favorable intraocular pressure reduction when combined with cataract surgery in the FDA-approved COMPASS trial 2). However, a post-marketing study at 5 years postoperatively revealed a significant decrease in corneal endothelial cell density compared to the cataract surgery-alone group 3). The number of retention rings protruding into the anterior chamber showed a negative correlation with corneal endothelial cell loss. As a result, it was voluntarily withdrawn from the market in August 2018 2)3).
Overall, MIGS has been reported to reduce intraocular pressure by 15–50% and decrease the number of medications by 0.4–1.8 agents 4). Combination with cataract surgery has shown additional intraocular pressure reduction (2–2.8 mmHg) and lower reoperation rates (3% vs 24% at 2 years) compared to MIGS alone 4). Suprachoroidal MIGS creates an artificial cyclodialysis between the anterior chamber and the suprachoroidal space, increasing uveoscleral outflow3).
QWhy was CyPass withdrawn from the market?
A
The CyPass Micro-Stent showed favorable intraocular pressure reduction in the FDA-approved COMPASS trial, but a post-marketing study at 5 years postoperatively revealed a significant decrease in corneal endothelial cell density compared to the cataract surgery-alone group 2)3). The number of retention rings protruding into the anterior chamber was independently correlated with corneal endothelial loss. Due to this safety issue, the manufacturer Alcon decided on a voluntary recall in August 2018. This experience highlights the importance of minimizing the impact of anterior chamber structures on the corneal endothelium in the design of suprachoroidal devices.
6. Pathophysiology and Detailed Mechanism of Onset
Aqueous humor is produced in the ciliary body and exits the eye via two pathways. The main pathway, the trabecular meshwork-Schlemm’s canal pathway, accounts for 80–95% of total outflow, while the secondary pathway, the uveoscleral pathway, accounts for 5–20%.
Outflow through the main pathway is pressure-dependent and increases with rising intraocular pressure. Outflow through the secondary pathway is pressure-independent 5). Aqueous humor passes through the ciliary stroma into the suprachoroidal space, then exits via the sclera into orbital vessels 5).
Suprachoroidal devices create an artificial communication between the anterior chamber and the suprachoroidal space. This increases outflow through the secondary uveoscleral pathway, thereby lowering intraocular pressure3).
In essence, they create a microscopic cyclodialysis, a principle identical to Heine’s cyclodialysis from 1905. Traditional cyclodialysis was plagued by spontaneous closure of the cleft or uncontrolled hypotony, but modern devices aim to achieve controlled, sustained outflow.
The IOP-lowering limit of MIGS, similar to conventional trabecular meshwork/Schlemm’s canal-targeting devices, is constrained by distal outflow resistance and episcleral venous pressure 3). Mild to moderate open-angle glaucoma is the primary indication; for severe cases requiring substantial IOP reduction, bleb-forming surgery is recommended 3).
QHow does the uveoscleral outflow pathway function?
A
Aqueous humor flows from the anterior chamber through the interstitium of the ciliary body and iris root into the suprachoroidal space. From there, it is reabsorbed by scleral vessels and choroidal capillaries, and also exits through scleral pores to the episclera 5). This pathway, unlike the main trabecular meshwork-Schlemm’s canal pathway, is pressure-independent and accounts for 5–20% of total aqueous outflow. Prostaglandin analogs lower IOP by increasing outflow through this pathway. Suprachoroidal devices create an artificial cyclodialysis, directly increasing outflow into this secondary pathway.
After the market withdrawal of the CyPass Micro-Stent, the field of suprachoroidal MIGS is advancing in the following directions:
MINIject, developed by iSTAR Medical, is the only intraocular suprachoroidal MIGS device listed in the EGS guidelines 1)
Bio-interventional cyclodialysis (CycloPen™) is a new technique that uses an allograft to reinforce the cleft and prevent re-occlusion, and its design does not protrude into the anterior chamber, avoiding impact on the corneal endothelium.
Standardization of clinical endpoint reporting for MIGS is underway, which is expected to enable accurate comparisons between devices 3)
Future challenges include the following.
Accumulation of long-term safety data on the corneal endothelium
Direct comparative trials of suprachoroidal devices and trabecular meshwork-targeting devices
Large-scale clinical trials of bio-interventional cyclodialysis
Optimization of anterior chamber structures in device design (minimizing impact on corneal endothelium)
QAre there any currently available suprachoroidal devices?
A
After the CyPass Micro-Stent was withdrawn from the market in 2018, MINIject (iSTAR Medical) is the only device for suprachoroidal MIGS via an intraocular approach 1). The GMS with an extraocular approach was approved in some countries, but clinical outcomes varied and it has not been widely adopted. As a new technique, bio-interventional cyclodialysis (allograft reinforcement with CycloPen™) is being developed and is attracting attention as a suprachoroidal approach without device implantation.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.
Fellman RL, Mattox CG, Ross C, et al. Reporting Clinical Endpoints in Studies of Minimally Invasive Glaucoma Surgery. Ophthalmology. 2025;132(2):141-159.
Singh P, Sharma B, Sarma N, Nag DS, Patnaik A, Verma R. Clinical Outcomes and Patient-Reported Outcomes of Minimally Invasive Glaucoma Surgery Techniques Over the Past Decade. Cureus. 2025;17(7):e87872. doi:10.7759/cureus.87872. PMID:40809659; PMCID:PMC12344473.
De Groef L, Bhatt DK, Bhatt AP, et al. The Role of Aqueous Humor Outflow Pathways in Glaucoma. Annu Rev Vis Sci. 2022.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.