Low vision is visual impairment due to eye disease, defined as best-corrected visual acuity in the better eye of 20/50 (0.4) or worse that cannot be improved by conventional means3). Even if visual acuity is better than 20/50, low vision may be present if accompanied by visual field loss, reduced contrast sensitivity, or increased glare.
Glaucoma is the most common cause of irreversible blindness worldwide1). As of 2020, the global number of glaucoma patients was estimated at 76 million, projected to reach 111.8 million by 20401). Open-angle glaucoma (OAG) has a higher prevalence than angle-closure glaucoma (ACG), but the proportion leading to blindness is higher for ACG (OAG about 10%, ACG about 25%)1).
Among glaucoma patients, 57% report needing more light, 55% report blurred vision, 46% report glare, 36% report significant visual field loss, and 30% report reduced contrast sensitivity. In glaucoma patients receiving visual rehabilitation, difficulties with reading (88%), writing (72%), and mobility (67%) are the most common.
QCan I receive low vision care even if I have glaucoma?
A
Yes. Although visual impairment from glaucoma is irreversible, low vision care can help you learn to maximize your remaining vision. Devices such as magnifiers, tinted glasses, improved lighting, and scanning training can improve reading, mobility, and daily activities. Ask your ophthalmologist for a referral to a low vision clinic.
In the early stages of glaucoma, there are often no subjective symptoms 4). As the disease progresses, patients may notice “partial blurriness” or “areas where objects cannot be recognized.” In more advanced stages, symptoms such as “overall blurriness” or “glare” are reported. Along with visual function decline including difficulty seeing, reduced visual acuity, whitish vision, and night blindness, daily life problems such as falling or bumping into objects occur.
Visual field defects: Glaucoma has traditionally been thought to primarily cause loss of peripheral vision, with central vision preserved until the end stage. However, recent evidence shows that in early glaucomatous damage, the macula is affected more frequently than previously thought 2).
Reduced contrast sensitivity: Damage to retinal ganglion cells in glaucoma leads to decreased contrast sensitivity2). Reduced contrast sensitivity and increased crowding effect contribute to narrowing of the visual span (number of characters recognized at a glance) and functional visual field 2).
Reading difficulty: Even when visual acuity is preserved, reading difficulties occur. Difficulty following lines, moving to the next line, reading small characters, and reduced reading speed (less than 80 words per minute) during sustained reading have been reported 2).
The root cause of low vision due to glaucoma is progressive degeneration of retinal ganglion cells and the associated optic neuropathy2). There is a clear correlation between the number of retinal ganglion cells and visual field sensitivity 2).
Functional Impairment
Associated Neural Damage
Peripheral visual field loss
Axonal damage at the superior and inferior lamina cribrosa
Central visual field defect
Ganglion cell damage in the macula
Reduced contrast
Functional abnormality of retinal ganglion cells
Risk factors for low vision include advanced age, advanced visual field loss, bilateral impairment, poor treatment adherence, and low educational level. When glaucoma patients subjectively notice visual field abnormalities, optic nerve damage is often already significantly advanced 4).
Low vision assessment evaluates functional visual abilities in addition to standard eye examinations.
Visual Acuity Testing: Use high-contrast visual acuity charts and bright illumination. Using a logMAR chart with 0.02 increments allows fine measurement, which is an advantage in low vision assessment. Projector charts are unsuitable because they have low contrast and are presented in a dark room.
Near Visual Acuity: Assess reading acuity for whole words using the Bailey-Lovie near reading card or similar. This is useful for prescribing reading aids.
Visual Field Testing: Evaluate the remaining visual field available for rehabilitation 4). The Goldmann perimeter uses large targets to facilitate assessment. The Humphrey Field Analyzer 10-2 program is useful for evaluating the remaining central visual field in end-stage glaucoma4).
Contrast Sensitivity: Use the Pelli-Robson contrast sensitivity chart or VISTECH contrast test. This is important for daily visual tasks such as recognizing faces, distinguishing pills, and detecting steps.
Use vision-related quality of life questionnaires (e.g., NEI-VFQ-25, GQL-15) to understand patients’ functional complaints 3). It is important to screen for visual impairment in glaucoma patients beyond clinical tests.
Ashley D Deemer; Judith E Goldstein; Pradeep Y Ramulu. Approaching rehabilitation in patients with advanced glaucoma. Eye (Lond). 2023 Jul;37(10):1993-2006. Figure 1. PMCID: PMC10333291. License: CC BY.
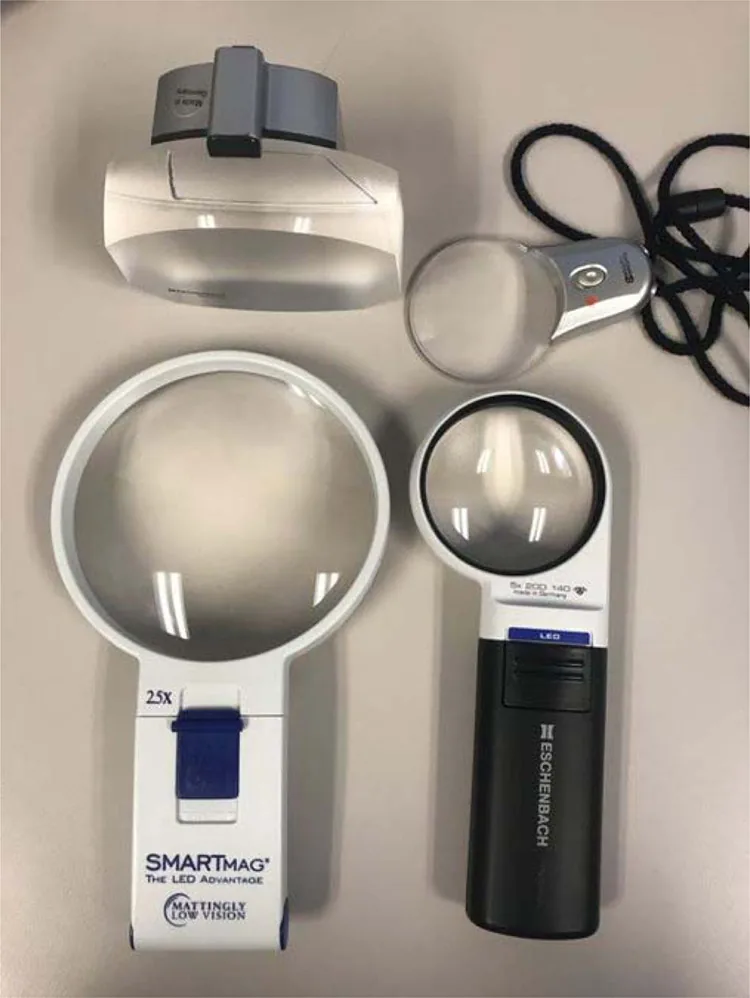
Examples of an illuminated desktop magnifier and a handheld magnifier. The image shows assistive devices that supplement text size and lighting conditions for near vision.
Near Magnification and Reading Support
Video magnifier (CCTV): Allows magnification adjustment, high contrast, and black-white inversion; it is the gold standard for low vision services.
Optical aids: Corrective, tinted, and low-vision glasses. Monocular telescopes are useful for viewing distant information.
Electronic devices: Tablets, smartphones, and computers can magnify images, increase contrast, and provide voice input/output.
Typoscope: A reading guide that helps follow lines. Signature guides and place markers are also useful.
Visual Field Enhancement and Mobility Support
Scanning training: Systematic exploration patterns such as head turning, eye scanning, and reducing approach speed are trained.
Eccentric viewing training: For patients with central scotoma, eccentric viewing training that utilizes peripheral vision is effective.
Mobility training: Training in the use of a white cane and safe indoor/outdoor movement is fundamental.
Glare control: Managed with tinted glasses, polarized lenses, anti-reflective coating, and lighting adjustments.
QDoes low vision care restore vision?
A
Low vision care is not a treatment that restores lost vision itself. Its goal is to maximize the use of remaining vision to improve daily functioning. Multiple studies have shown that video magnifiers, tinted glasses, scanning training, etc., improve the quality of reading, mobility, and activities of daily living.
In glaucoma, loss of retinal ganglion cells (RGCs) occurs at the lamina cribrosa of the optic nerve head 2). Anterograde and retrograde axonal transport in RGC axons is blocked, and the supply of neurotrophic factors is interrupted, leading to reactivation of programmed cell death (apoptosis).
Loss of RGCs also affects central visual function 2). RGC damage in the macular region leads to decreased contrast sensitivity, changes in spatial summation, and increased visual crowding, which collectively contribute to narrowing of the visual span and functional visual field 2). Conventional high-contrast single-letter visual acuity tests and standard automated perimetry may not adequately reflect patients’ actual visual function in daily life 2).
Many glaucoma patients have difficulty noticing their own scotomas 2). The visual system tends to fill in missing visual field information with surrounding information, which is one factor that makes early detection difficult.
Treatment outcomes of low vision care have been evaluated in multiple studies. After treatment, statistically significant improvements were observed in many categories including overall visual ability, reading, mobility, social functioning, and emotional well-being. Approximately half of patients who received LVS showed clinically meaningful improvement.
In a randomized trial of glaucoma patients, the group that received low vision examination and treatment showed significant improvements in reading ability and overall visual ability compared to the group that received examination only.
Recent studies have revealed that macular damage is more common in the early stages of glaucoma than previously thought 2). In visual tasks involving divided attention or time constraints, glaucoma patients show greater difficulty 2). Further research is needed on how central visual dysfunction in glaucoma affects reading and face recognition 2).
The biggest challenge in visual rehabilitation is the coordination between medical rehabilitation and independent living training/vocational training. It is expected that the nationwide development of low vision care networks (Smart Site) being established in each prefecture will facilitate this bridging more smoothly.
QWill I be unable to drive due to glaucoma?
A
It depends on the progression of glaucoma. Driving is possible if visual field impairment is mild, but increased difficulty, especially during nighttime driving, has been reported. Glaucoma patients are about three times more likely to stop driving due to subjective visual deficits. In Japan, there are visual field test standards when renewing a driver’s license, so please consult your doctor.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.
Kwon M. Glaucomatous Retinal Ganglion Cell Loss and Pattern Vision. Annu Rev Vis Sci. 2024;10:427-445.
Gedde SJ, Vinod K, Wright MM, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern. Ophthalmology. 2021 Jan;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022. PMID:34933745.