Intracranial hypertension
Headache: Tends to worsen when lying down.
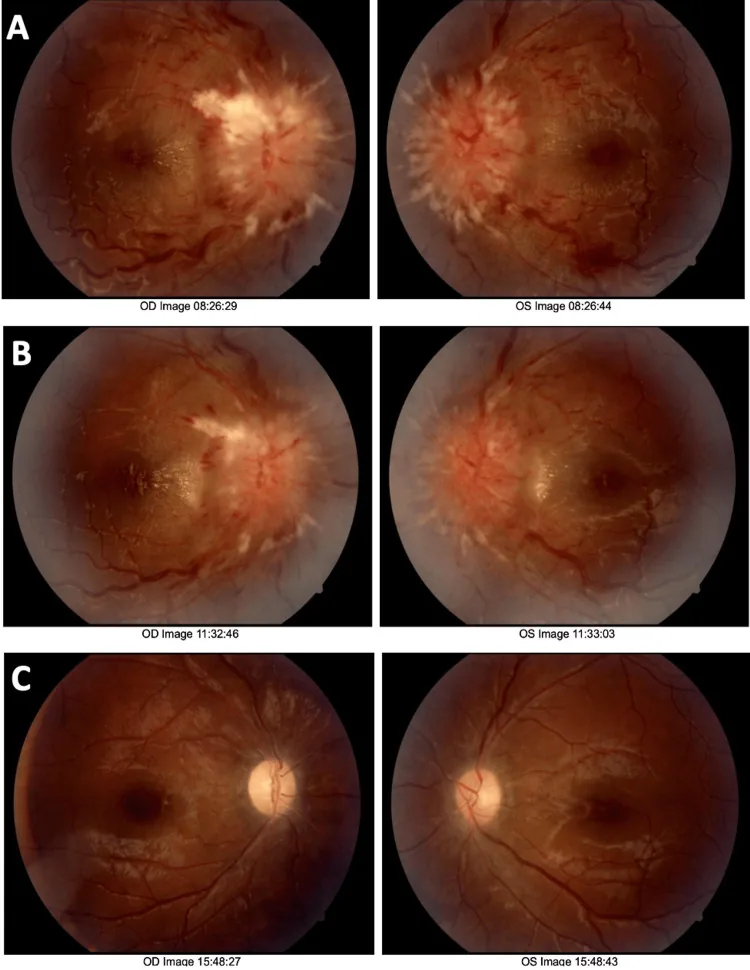
Papilledema: Suggests elevated intracranial pressure.
Cause: Shunt obstruction or malfunction.

Idiopathic intracranial hypertension (IIH) is a disease characterized by elevated intracranial pressure (ICP) of unknown cause. It predominantly affects obese women of reproductive age. The incidence of IIH is increasing worldwide 1).
The revised Dandy criteria are used for the diagnosis of IIH. The specific diagnostic requirements are as follows.
CSF diversion includes ventriculoperitoneal (VP) shunts and lumboperitoneal (LP) shunts. Both lower intracranial pressure in IIH, but shunting is often a temporary measure. LP shunt malfunction occurs relatively frequently, with an average time to failure reported as 5–10 years.
Because the clinical presentation is diverse, diagnosing delayed LP shunt malfunction can be difficult. Currently, many institutions have shifted to using VP shunts over LP shunts.
Many reports indicate that the average time to LP shunt malfunction is 5 to 10 years. However, individual differences are large depending on BMI and catheter type. For details, see the section on “Causes and Risk Factors”.
LP shunt failure presents with symptoms similar to IIH recurrence. The main symptoms and their frequencies are as follows.
Headache in IIH initially presents as an intracranial hypertension type that worsens upon waking, but over time it becomes chronic and often shows migraine-like features (with photophobia, phonophobia, and nausea) 1).
Papilledema is a typical finding in IIH, but it is not necessarily observed in LP shunt failure. It is usually bilateral and symmetric, but may be unilateral or asymmetric.
Clinical data in LP shunt dysfunction are as follows:
Visual field testing often reveals enlarged blind spots, nasal steps, and arcuate scotomas. In cases of long-term shunt failure, optic atrophy may occur.
The reasons for requiring LP shunt revision are diverse. The main causes are listed below.
The use of Silastic catheters dramatically reduced occlusion and fracture rates. As a result, the lifespan of LP shunts was further extended.
The relationship between BMI and shunt survival is shown below.
| BMI | Median shunt survival |
|---|---|
| <25.0 (healthy) | 44 months |
| High BMI | 18 months |
In obese patients, technical difficulty in placing the catheter under the peritoneum is considered a factor in shortened survival.
Children have a higher risk of complications due to increased mechanical stress, changes in intrathecal tube size, and relative shortening of the catheter with growth. Therefore, delayed LP shunt failure is more common when the initial placement occurs in adulthood.
As risk factors for IIH itself, obesity and weight gain are the largest modifiable factors 2). Endocrine disorders (Addison’s disease, hypoparathyroidism, steroid withdrawal) are also involved in the development of IIH 2).
In patients with a BMI below 25.0, the median shunt survival is 44 months, whereas in high-BMI patients it is only 18 months. Technical difficulties in catheter placement are considered a contributing factor in obese patients.
In patients who have previously undergone LP shunt surgery, identifying the cause of recurrent symptoms relies on medical history and physical examination. The following tests are combined for evaluation.
The following ophthalmologic examinations are performed:
Other causes of increased intracranial pressure besides LP shunt failure must be excluded.
Differentiating between overdrainage (intracranial hypotension) and shunt failure (intracranial hypertension) is particularly important. Symptoms of both conditions overlap.
Intracranial hypertension
Headache: Tends to worsen when lying down.
Papilledema: Suggests elevated intracranial pressure.
Cause: Shunt obstruction or malfunction.
Intracranial Hypotension
Headache: Tends to worsen when standing.
Papilledema: Usually not present.
Cause: Excessive CSF drainage due to shunt.
Abducens nerve palsy, blurred vision, and headache can occur with both overdrainage and underdrainage, so caution is needed.
In intracranial hypertension, headache worsens in the supine position and is often accompanied by papilledema. In contrast, in intracranial hypotension, headache worsens in the upright position. However, since abducens nerve palsy and diplopia can occur in both conditions, measurement of opening pressure via lumbar puncture is important for differentiation.
Treatment of LP shunt failure usually requires shunt revision or replacement.
Many institutions prefer VP shunt as the CSF diversion procedure for IIH. The reasons are as follows:
VP shunt surgery has been reported to improve or stabilize vision in patients with rapidly worsening vision or in IIH patients with progressive visual impairment despite medical therapy or optic nerve sheath fenestration (ONSF).
In the UK, the use of ICP monitors, programmable valves, and anti-siphon valves is recommended1).
ONSF is an option when medical treatment fails or when shunt reconstruction is not possible. It is suitable for patients with mild headache but severe visual decline and persistent optic disc edema1).
Focal venous stenosis is found in 30–93% of IIH patients. Candidates are those with focal stenosis of the transverse or sigmoid sinus.
For IIH, weight loss and a low-salt diet are recommended. Bariatric surgery has been shown to result in sustained reduction of ICP and weight loss 1). A 24% reduction in body weight is reported to lead to disease remission, but even a 5–15% weight loss is beneficial for resolution of papilledema 1).
Currently, many institutions prefer VP shunts. Compared to LP shunts, VP shunts have lower complication and revision rates, and tend to result in shorter hospital stays in the event of shunt failure.
The exact mechanism of ICP elevation in IIH is not fully understood. Dysregulation of CSF dynamics and involvement of metabolic and hormonal factors have been suggested2).
The relationship between ICP and intracranial volume is shown by an S-shaped pressure-volume curve. For volume increases up to 30 cm³, compensatory mechanisms (such as displacement of intracranial venous blood) result in only minor ICP changes. Once compensatory mechanisms are exhausted, even a small volume increase can cause a steep rise in ICP2).
IIH is a multifactorial disease involving both genetic and environmental factors2).
The causes of delayed LP shunt dysfunction are multifactorial.
Venous stent placement is attracting attention as a new treatment option for IIH.
In the UK, a randomized controlled trial (RCT) comparing venous stent placement with shunt surgery is ongoing1). Eligible patients are those with venous stenosis and proven pressure gradient who are intolerant or unresponsive to medical therapy. A drawback is the need for antiplatelet therapy for 6 months after surgery.
The following areas have been identified as priority research topics in IIH2).
Toshniwal et al. (2024) pointed out that existing drugs such as acetazolamide may show only limited efficacy in lowering ICP, and stated that the search for new drug targets is urgent 2). Refinement of preclinical research is considered essential for understanding the pathophysiology of IIH and expanding treatment options.