Brittle cornea syndrome (BCS; OMIM 229200, 614170) is a rare autosomal recessive connective tissue disorder characterized by progressive corneal thinning and blue sclera. It was first reported by Stein et al. in 19682). The prevalence is estimated to be less than 1 per 1,000,000 people1). As of 2021, a total of 86 cases have been reported, with many cases having a family history of consanguineous marriage1).
BCS is classified into two types based on the causative gene1). Both types encode transcription factors involved in maintaining extracellular matrix homeostasis1)2). Impaired collagen deposition and fiber assembly lead to structural fragility of the corneal stroma1).
Number of reported patients: 53 cases (24 mutations identified)1)
Main mutation types: Mostly homozygous frameshift or nonsense mutations1)
Special note: Heterozygous mutations have been reported to be associated with keratoconus2)
BCS type 2 (PRDM5 mutation)
Causative gene: PRDM5 (4q27) is a 16-exon gene encoding 630 amino acids1)
Number of reported patients: 33 cases (14 different mutations identified)1)
Main mutation types: All reported as homozygous mutations1)
Special note: Also involved in the development of retinal microvessels and Bruch’s membrane1)
QHow does BCS differ from Ehlers-Danlos syndrome?
A
BCS was previously considered part of kyphoscoliotic Ehlers-Danlos syndrome (EDS type VI). However, molecular genetic analysis has confirmed it to be a distinct disease1). EDS VI is caused by lysyl hydroxylase deficiency due to PLOD1 gene mutations. It can be differentiated by an elevated urinary deoxypyridinoline/pyridinoline ratio, which is normal in BCS1). EDS VI has a poor prognosis due to arterial rupture, whereas the life expectancy in BCS is considered normal.
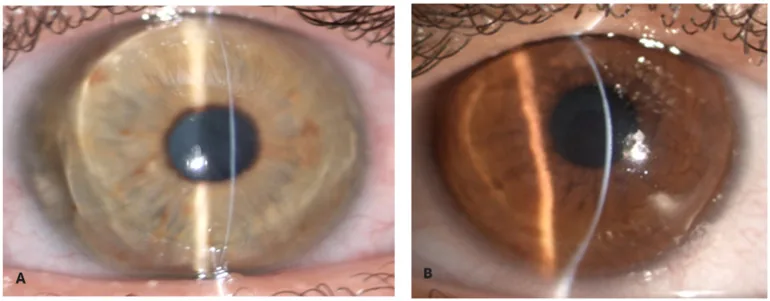
Zeppieri M, Nabil R, Ruzza A, et al. Brittle Cornea Syndrome: Molecular Diagnosis and Management. Diagnostics (Basel). 2025 Jun 24;15(13):1596. Figure 1. PMCID: PMC12249002. License: CC BY.
With a narrow slit-lamp beam, the corneal stroma appears extremely thin and bulges forward. The extreme thinning and conical protrusion show the appearance of a fragile cornea.
Progressive myopia and visual loss due to irregular astigmatism are the main complaints3). Sudden pain and vision loss occur at the time of corneal perforation5). Hearing loss due to deafness may also be noticed1).
Thinning of the entire cornea (from limbus to limbus) is most characteristic. Central corneal thickness (CCT) is often less than 400 μm1). In a report of three siblings, CCT was 243–304 μm5). In Albanian siblings, it was 189 μm and 157 μm3). In two brothers from New Zealand, extreme thinning of 167 μm and 149 μm was confirmed4).
Corneal perforation occurs at an average age of 4.3 years (range 1.5–19 years) 1). Ocular perforation is observed in more than two-thirds of reported cases 1). Permanent vision loss occurs in more than half of cases 1). Blue sclera is the most frequent ocular finding, observed in 72 of 78 cases 1).
System
Main findings
Frequency
Ocular
Corneal thinning/perforation, blue sclera
>90% 1)
Joint
Small joint hypermobility
64/78 cases 1)
Auditory
Sensorineural, conductive, or mixed hearing loss
32/78 cases 1)
Joint hypermobility is the most frequent extraocular finding 1). Congenital hip dysplasia, scoliosis, and flat feet have also been reported 1). Hearing loss tends to affect higher frequencies more severely 1). Hypercompliance of the tympanic membrane is characteristic 1). The skin is soft, hyperextensible, and prone to easy bruising 1).
Reports of bone fragility have also increased in recent years. Two brothers with compound heterozygous ZNF469 mutations had more than 10 fractures and osteopenia 4). It has been suggested that approximately 16% of BCS patients may have bone fragility 4). Bone biopsy showed thinning of cortical bone and a marked decrease in cortical bone porosity 4).
BCS is an autosomal recessive disorder caused by biallelic mutations in two genes 1).
ZNF469 is involved in the normal development of the anterior chamber and cornea1). Genome-wide association studies have shown an association with central corneal thickness 4). PRDM5 directly regulates the transcription of fibrillar collagen genes 4). Loss-of-function mutations (frameshift and nonsense mutations) account for a high proportion of mutations in both genes 1).
Heterozygous mutations in ZNF469 are associated with reduced central corneal thickness 2). However, they do not necessarily lead to corneal thinning. A 64-year-old Chinese male with a heterozygous ZNF469 mutation had normal corneal thickness (approximately 550 μm) but presented with corneal opacity and epithelial defects 2).
Consanguineous marriage is an important risk factor, increasing the probability of homozygous mutations 1). In three Turkish cases, a common PRDM5 c.17T>G, p.(Val6Gly) mutation was identified, suggesting a possible founder mutation 1).
Clinical diagnosis is made based on generalized corneal thinning (central corneal thickness less than 400 μm), blue sclera, and systemic symptoms such as joint hypermobility and hearing loss 3). Corneal pachymetry and corneal topography using devices such as Pentacam are essential 3). Anterior segment OCT is useful for detailed evaluation of corneal structure 2)3).
Genetic testing of ZNF469 and PRDM5 is necessary for a definitive diagnosis 3). Whole exome sequencing (WES) is effective for identifying pathogenic variants 3). It also provides useful information for genetic counseling and family planning 3). Carriers may develop myopia and mild corneal thinning 2).
In BCS, differentiation from kyphoscoliotic EDS (kEDS-PLOD1) is particularly important. In kEDS-PLOD1, when ocular rupture occurs, the sclera is more prone to rupture than the cornea1). In kEDS-PLOD1, scoliosis, hypotonia, and vascular complications are more prominent1).
QWhy is early diagnosis of BCS important?
A
The average age of onset of corneal perforation is 4.3 years, and surgical repair after perforation is extremely difficult5). More than half of reported cases result in permanent vision loss1). Early diagnosis allows for protective eyewear and trauma prevention education1). Screening of siblings is also important for early detection5).
The most important aspect of BCS management is prevention of corneal perforation1). Continuous use of polycarbonate protective eyewear is recommended5). Prophylactic use of intraocular pressure-lowering medications may also be considered. Contact lenses are restricted due to corneal thinning and risk of trauma1).
Outcomes: Best corrected visual acuity (BCVA) improved from 20/200 to 20/30 and 20/25 in Albanian siblings 3)
Course: No complications occurred over 7 years 3)
Deep Anterior Lamellar Keratoplasty (DALK)
Advantages: Preserving the endothelium reduces the risk of rejection 3)
Limitations: Risk of intraoperative perforation due to stromal fragility 3)
Reported case: In one case, central endothelial perforation occurred intraoperatively and was converted to PKP3)
Selection criteria: Adequate stromal thickness and integrity of Descemet’s membrane are required 3)
In corneal perforation repair, extreme tissue fragility is a problem. In a report of three siblings, the use of long suture bites, cyanoacrylate adhesive, and a bandage contact lens was effective 5). Careful creation of a corneoscleral tunnel can reduce complications 5). A 64-year-old BCS patient underwent PKP and had a corrected visual acuity of 0.2 at discharge 2).
QIs corneal collagen cross-linking effective?
A
Two pediatric BCS patients with central corneal thickness less than 280 μm underwent transepithelial CXL (UV irradiation dose adjusted for corneal thickness) 3). Improvement in visual acuity and maintenance of endothelial cell density were reported 3). However, the standard Dresden protocol requires a central corneal thickness of at least 400 μm, and it is contraindicated for ultrathin corneas less than 200 μm 3). Protocol modifications are expected to expand the indications, but currently it is limited.
Both ZNF469 and PRDM5 encode transcription factors 1). ZNF469 has three C2H2-type zinc finger domains at the C-terminus 1). It regulates the expression of extracellular matrix genes (CLU, GPC6, PCOLCE2, THBS1) 1). PRDM5 has a PR SET domain and directly regulates transcription of collagen genes via binding to RNA polymerase II 4). It is also involved in the regulation of the Wnt signaling pathway.
These genetic mutations impair collagen deposition and fiber assembly in the corneal stroma1). ZNF469 mutations cause reduced expression and structural changes of type I collagen (COL-I) 2). Immunofluorescence staining of corneal tissue after PKP demonstrated decreased COL-I and increased type III collagen 2). Masson staining also showed a clear reduction in collagen fiber content 2).
Confocal microscopy reveals highly reflective reticular striae in the anterior corneal stroma2). There is no accompanying inflammatory cell infiltration 2). This suggests that corneal lesions in BCS result from a primary abnormality in collagen structure.
In bone tissue, PRDM5 also binds to exon DNA of type I collagen genes 4). Bone biopsy showed thinning of cortical bone and a marked reduction in cortical porosity (1.3%; normal 6.3±0.6%) 4). A 28-gene bone fragility panel detected no other pathogenic mutations, suggesting that ZNF469 mutations themselves may cause bone fragility 4).
QWhy are non-corneal tissues affected in BCS?
A
ZNF469 and PRDM5 are involved in transcriptional regulation of extracellular matrix in connective tissues throughout the body 1). Structural abnormalities of collagen fibers are not limited to the cornea but affect systemic connective tissues including the sclera (blue discoloration), joints (hypermobility), skin (hyperextensibility), bone (osteopenia), and tympanic membrane (hypercompliance) 4). Reports of osteopenia and fractures suggest that BCS may have a bone fragility phenotype 4).
Advances in gene therapy are opening new possibilities for BCS. CRISPR genome editing and RNA interference (RNAi) are expected as treatments aimed at stabilizing or improving corneal thinning 3).
Bioengineered corneal implants (BPCDX) are acellular transparent hydrogels made from medical-grade porcine collagen 3). They are inserted into a 2–3 mm intrastromal pocket created by femtosecond laser, a minimally invasive procedure 3). At 24 months, increased corneal thickness, flattening of maximum keratometry by 18 D, and improved corrected visual acuity have been reported 3). Stable results without rejection have been achieved 3).
Intrastromal injection of mesenchymal stem cells is also being studied 3). Adipose-derived and bone marrow-derived stem cells are injected into a lamellar dissection created by femtosecond laser, potentially delaying the need for PKP3). Currently used only in keratoconus patients, but application to BCS patients is expected 3).
Sanri A, Demir S, Gürkan H. Homozygous Val6Gly Variation in PRDM5 Gene Causing Brittle Cornea Syndrome: A New Turkish Case. Mol Syndromol. 2023;14(2):129-135. doi:10.1159/000524832. PMID:37064337; PMCID:PMC10091010.
Geng X, Zhu L, Li J, Li Z. Brittle cornea syndrome: A novel mutation. Heliyon. 2024;10:e32506. doi:10.1016/j.heliyon.2024.e32506.
Zeppieri M, Gentile M, Acquaviva A, Scollo D, D’Esposito F, Gagliano G, et al. Brittle Cornea Syndrome: Molecular Diagnosis and Management. Diagnostics (Basel, Switzerland). 2025;15(13). doi:10.3390/diagnostics15131596. PMID:40647596; PMCID:PMC12249002.
Cundy T, Vincent A, Robertson S. Does brittle cornea syndrome have a bone fragility phenotype? Bone Rep. 2021;15:101124. doi:10.1016/j.bonr.2021.101124. PMID:34522702; PMCID:PMC8426531.
Mandlik K, Betdur RA, Rashmita R, Narayana S. Brittle cornea syndrome: A tale of three brothers. Indian journal of ophthalmology. 2022;70(7):2594-2597. doi:10.4103/ijo.IJO_2894_21. PMID:35791165; PMCID:PMC9426125.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.