Strabismus Fixus is a progressive, large-angle esotropia and hypotropia with restricted ocular rotation that develops in patients with long-standing pathological high myopia. It is also known as “Heavy eye syndrome.” It is considered the most severe form of age-related divergence insufficiency.
High myopia is generally defined as a refractive error of -8.00D or more and an axial length of 27 mm or more. In most cases of fixed strabismus, the axial length reaches 30 mm or more. It occurs in association with congenital fibrosis, amyloidosis, high myopia, etc.
The age of onset is often middle-aged or older, and the course is progressive. There is a marked sex difference, with women accounting for about 90% of cases.
The global increase in the prevalence of myopia is also an important background. By 2050, the world’s myopic population is expected to increase to about 5 billion, and the high myopia population to about 1 billion7). In Japan, a survey of 22,379 people in their 60s and 70s reported that 6.96% had high myopia with an axial length of 26.0 mm or more in both eyes1), and the prevalence of high myopia (-7.90D) has increased from 0.2% to 1.6% over 30 years1).
QWhat kind of people are more likely to have fixed strabismus?
A
It is more common in elderly women with high myopia. About 90% of patients are women, and the majority have an axial length of 30 mm or more. It typically develops after middle age and progresses gradually.
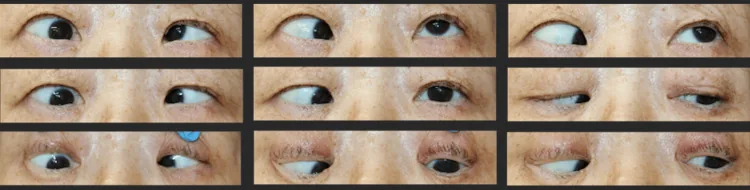
Koiwa C, et al. A Case of Strabismus Fixus With Extremely Long Axial Length Results in Improvement of Limitation of Abduction by the Yokoyama Procedure. Cureus. 2024. Figure 1. PMCID: PMC11090074. License: CC BY.
In multiple gaze directions, the right eye is deviated inferomedially, with severe restriction of abduction and elevation. This photograph shows the characteristic ocular position abnormality and eye movement disorder seen in fixed strabismus (high myopic strabismus).
The eye is fixed in an adducted and infraducted position; in the most severe cases, it does not move at all. Mechanical restriction of movement is observed in abduction and supraduction. The traction test is positive in the abduction and supraduction directions.
There are two main phenotypes of fixed strabismus2).
Esotropia and Hypotropia Type
Eye position: Mainly inward and downward deviation. The most common phenotype.
Abduction limitation: Eye movement in the outward direction is significantly restricted.
Elevation limitation: Upward eye movement is also impaired.
Strabismus angle: In typical cases, esotropia reaches about 110 PD and hypotropia 14 PD2).
Exotropia and Hypotropia Type
Eye position: Mainly outward and downward deviation. A relatively rare phenotype.
Adduction limitation: Eye movement in the adduction direction is restricted.
Differences in pathogenesis: The patterns of downward displacement of the lateral rectus and nasal displacement of the superior rectus differ.
Associated findings: May be accompanied by a yellowish, soft fatty mass under the conjunctiva (fat prolapse)2).
When accompanied by subconjunctival fat prolapse, it is observed as a yellowish, soft mass under the superolateral conjunctiva2).
High myopic strabismus fixus: The mean axial length in myopic strabismus fixus varies by report: 28.9±2.03 mm, 30.5±3 mm, and 32±5 mm 1). In many patients, myopia is -15 D or more and axial length exceeds 31 mm 2).
QDoes high myopia always lead to strabismus fixus?
A
Not all patients with high myopia develop strabismus fixus. If axial elongation occurs in a uniform direction and dislocation of the eyeball superolaterally does not occur, strabismus fixus does not develop. The relationship between the direction of axial elongation and the muscle cone is key to pathogenesis.
Orbital MRI coronal sections are the most suitable diagnostic method. T1-weighted imaging (without fat suppression) is optimal, clearly evaluating extraocular muscle displacement and posterior globe dislocation.
Measurement of the dislocation angle (SR-LR angle) is important, reaching an average of 179.9±30.8° in fixed strabismus, which is significantly larger than the average of 102.9±6.8° in cases without fixed strabismus 4). In mild cases, MRI in multiple directions (forward gaze, right-downward, left-downward) is necessary.
Coronal CT can also evaluate the dislocation position of the posterior eyeball and the condition of extraconal fat 2).
Differentiation from the following diseases is important.
Acquired bilateral abducens nerve palsy: Intracranial lesions must be ruled out.
Orbital trauma: Check for a history of trauma.
Thyroid eye disease: Differentiate using thyroid function tests and imaging findings.
Sagging eye syndrome: Presents with age-related abduction limitation but no globe dislocation.
QWhat imaging studies are useful for diagnosing fixed strabismus?
A
Coronal orbital MRI is most suitable. T1-weighted imaging (without fat suppression) evaluates extraocular muscle displacement and globe dislocation. In fixed strabismus, the dislocation angle between the superior rectus and lateral rectus averages 179.9±30.8°, significantly larger than in cases without fixed strabismus 4).
Surgery is the only effective treatment. Because the deviation is large and incomitant, conservative treatments such as prisms are generally not indicated.
This is the first-choice procedure. The muscle bellies of the superior rectus (SR) and lateral rectus (LR) are sutured and fixed 15 mm posterior to their insertions, aiming to return the dislocated posterior globe into the normal muscle cone. Standard suture material is 5-0 polyester.
Whether to add medial rectus recession to the Yokoyama procedure is debated. In cases with long-standing abduction limitation, medial rectus contracture may have occurred, so adding medial rectus recession may be recommended 1). However, some reports indicate no additional benefit of medial rectus recession compared to pure Yokoyama procedure, and others point out a risk of overcorrection 1).
Koiwa et al. (2024) reported a case of a 68-year-old woman with an extremely long axial length of 33.97 mm 1). Preoperatively, the right eye was fixed in adduction and infraduction, presenting with approximately 113Δ esotropia. MRI showed a dislocation angle of 181°. After Yokoyama procedure (suturing SR-LR 15 mm posterior to the insertion with 5-0 polyester suture) combined with 5 mm medial rectus recession, residual esotropia improved to about 20Δ, and abduction beyond midline became possible. Postoperative MRI showed improvement of the dislocation angle from 181° to 104°.
As an alternative to suture muscle fixation, loop muscle fixation using a silicone band is available 2). Compared to conventional suture muscle fixation, it has advantages of fewer complications such as globe perforation, muscle dehiscence, suture-related complications, and anterior segment ischemia 2)6).
Lalwani & Kekunnaya (2021) reported a 60-year-old male with bilateral high myopic fixed strabismus (axial length: right eye 34.21 mm, left eye 34.41 mm) complicated by fat prolapse 2). Surgery combining lateral rectus-superior rectus fixation with a silicone band (No. 240), medial rectus recession, and fat excision was performed. Postoperatively, abduction limitation improved from -4 to -1, and fat prolapse resolved 2).
Management of Deep Orbit and Narrow Palpebral Fissure (Modified Technique)
In cases with a deep orbit or narrow palpebral fissure, suturing 15 mm posterior to the insertion may be difficult with the conventional method. A modified technique adding lateral canthotomy, lateral canthal ligament disinsertion, and superior conjunctival fornix incision has been reported to secure a wider surgical field 3).
Lee et al. (2021) performed the modified Yokoyama procedure on a 69-year-old female with a deep orbit and narrow palpebral fissure (Hertel values 11 and 12 mm) 3). In addition to lateral canthotomy, partial removal of the lateral orbital wall ensured an adequate surgical field. At 3 months postoperatively, good ocular alignment and improvement in extraocular muscle movement were achieved 3).
QAre there any treatments for fixed strabismus other than surgery?
A
Surgery is the only effective treatment. Because the deviation is large and incomitant, conservative treatments such as prisms are generally not indicated. In addition to the difficulty of prism correction due to the angle of strabismus, the essence of treatment is to release the mechanical restriction of the eye, so no fundamental improvement can be expected without surgery.
The mechanism of high myopic strabismus fixus involves the following stepwise changes.
Axial elongation: As myopia progresses, the axial length increases, leading to staphylomatous changes at the posterior pole.
Rupture of the SR-LR band: As the eyeball enlarges, the intermuscular membrane (including supporting tissues such as Lockwood’s ligament) between the superior rectus and lateral rectus muscles stretches and ruptures.
Dislocation of the posterior globe: The posterior part of the eyeball dislocates from between the superior rectus and lateral rectus muscles out of the muscle cone, protruding superolaterally outside the muscle cone.
Deviation of extraocular muscles: The lateral rectus muscle deviates downward (converting abduction force into depression), and the superior rectus muscle deviates nasally (converting elevation force into adduction) 2). As a result, the eye is pulled into an adducted and depressed position.
Establishment of mechanical fixation: Chronic dislocation leads to contracture and fibrosis of the medial rectus muscle, resulting in mechanical fixed strabismus.
In highly myopic eyes without fixed strabismus, the average dislocation angle is 102.9±6.8°, whereas in fixed strabismus it is significantly larger at 179.9±30.8°4), indicating that the degree of dislocation is directly involved in the development of fixed strabismus.
General pathology: Histological findings of extraocular muscles show loss of myofibrils and fibrosis. In congenital fixed strabismus, congenital fibrosis of the medial rectus muscle is the main pathological finding; in cases secondary to lateral rectus palsy, secondary contracture and fibrosis of the medial rectus muscle are predominant.
7. Latest Research and Future Perspectives (Research Stage Reports)
Wabbels et al. (2021) reported real-world clinical data of the Yokoyama procedure in a large-scale multicenter analysis5). The addition of medial rectus recession was found to have no additional effect compared to the pure Yokoyama procedure, and the risk of overcorrection was also pointed out1). These results have deepened discussions on determining the indications for the surgical technique.
Increase in myopia population and future challenges
The global increase in the prevalence of myopia is predicted to lead to an increase in the number of patients with fixed strabismus1). With the high myopia population expected to reach approximately 1 billion by 20507), research on prevention and early intervention for fixed strabismus will become an important future issue.
The effectiveness of modified techniques for anatomically challenging cases such as deep orbits or narrow palpebral fissures has been reported3), and combining lateral canthotomy or partial removal of the lateral orbital wall may expand surgical indications. Additionally, ongoing studies are evaluating the combination of silicone band myopexy and fat resection for cases with fat prolapse2).
Koiwa C, Negishi T, Sakemi F, et al. A Case of Strabismus Fixus With Extremely Long Axial Length Results in Improvement of Limitation of Abduction by the Yokoyama Procedure. Cureus. 2024;16(4):e58194.
Lalwani S, Kekunnaya R. Bilateral myopic strabismus fixus with fat prolapse treated by silicone band loop myopexy and excision of fat. BMJ Case Rep. 2021;14:e238364.
Lee PA, Kono S, Kakizaki H, Takahashi Y. Modified Loop Myopexy (Yokoyama’s Procedure) for High Myopic Strabismus Fixus. Case Rep Ophthalmol. 2021;12:68-72.
Yamaguchi M, Yokoyama T, Shiraki K. Surgical procedure for correcting globe dislocation in highly myopic strabismus. Am J Ophthalmol. 2010;149:341-346.e2.
Wabbels B, Fricke J, Schittkowski M, et al. Yokoyama procedure for esotropia associated with high myopia: real-world data from a large-scale multicentre analysis. Acta Ophthalmol. 2021;99:e1340-e1347.
Shenoy BH, Sachdeva V, Kekunnaya R. Silicone band loop myopexy in the treatment of myopic strabismus fixus: surgical outcome of a novel modification. Br J Ophthalmol. 2015;99:36-40.
Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123:1036-1042.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.