Anton Syndrome is a condition of visual anosognosia in which patients with cortical blindness are unaware of their vision loss and describe nonexistent visual experiences. Despite being blind, they engage in confabulation, providing detailed descriptions of what they claim to see.
The condition is named after Austrian neurologist Gabriel Anton, who reported a 69-year-old case with acquired anosognosia and deafness due to bilateral temporal lobe lesions. The term “anosognosia” was coined by Joseph Babinski, so it is also called Anton-Babinski syndrome. The first description of visual anosognosia dates back to the Roman slave Harpaste, who denied her blindness and complained that the room was dark.
Difference from Charles Bonnet Syndrome: It is important to note that Charles Bonnet syndrome involves visual hallucinations in patients with visual impairment, but insight into the visual impairment is preserved, fundamentally differing from Anton syndrome.
Epidemiology: The median age is 55 years (range 6–96 years), with no sex difference. The most common cause is secondary to cerebrovascular accident (CVA), often in elderly patients with multiple vascular risk factors. Posterior cerebral artery (PCA) stroke accounts for 5–10% of all strokes. 1) Between 1965 and 2016, only 28 cases of Anton-Babinski syndrome were reported, making it extremely rare. 2)
QHow is Anton syndrome different from Charles Bonnet syndrome?
A
Anton syndrome is a condition in which patients with cortical blindness deny their own blindness and confabulate, lacking insight. In contrast, Charles Bonnet syndrome involves visual hallucinations in visually impaired patients, but they retain insight into their visual impairment. Both conditions have visual impairment as a background, but they fundamentally differ in the presence or absence of anosognosia.
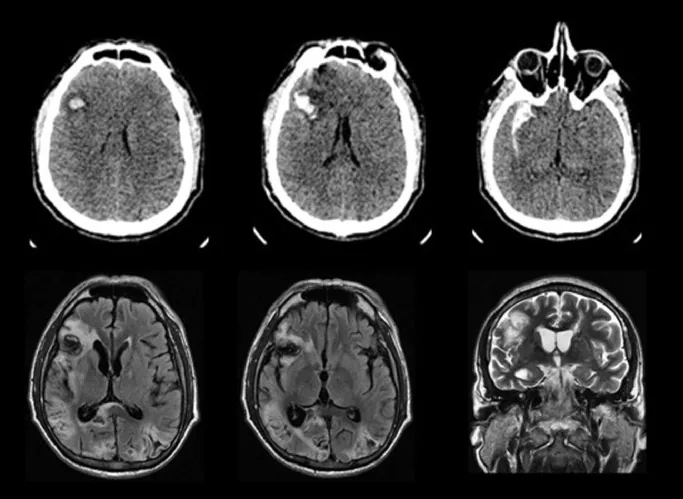
CT and MRI images of bilateral occipital lobe infarction causing Anton syndrome
Ricardo BM, et al. Anton syndrome after subarachnoid hemorrhage and delayed cerebral ischemia: A case report. Cereb Circ Cogn Behav. 2021. Figure 1. PMCID: PMC9616440. License: CC BY.
CT image shows hemorrhage and hematoma in the right frontal lobe, and MRI FLAIR and T2-weighted images show hemorrhagic infarction in both occipital lobes. This corresponds to bilateral occipital lobe infarction discussed in the section “2. Main Symptoms and Clinical Findings.”
Denial of vision loss: The patient does not recognize their own vision loss. Even when bumping into objects, they attribute it to external factors such as a dark room.
Confabulation: Detailed descriptions of nonexistent people or situations. When asked to shake hands, they reach in the wrong direction.
Partial preservation of color vision: Color vision may be preserved. Moving objects can be recognized, but stationary objects may be difficult to recognize. This is due to a subcortical fiber pathway that bypasses V1 to reach area V5. 1)
Clinical Findings (Findings Confirmed by Physician Examination)
Visual acuity: Complete loss (NLP: no light perception), but the patient is unaware.
Pupillary reflex: Normal. Occipital lobe lesions are located posterior to the lateral geniculate body, so they do not affect the pupillary pathway. The afferent pathway for the light reflex goes to the pretectal area of the midbrain before the lateral geniculate body.
Fundus examination: Normal. No organic abnormalities are found within the eye. 1)
Threat reflex: Negative.
Eye movements: Follows verbal commands normally, but unable to visually track.
Corneal reflex: Normal (independent of cortical input).
Riddoch phenomenon: Unable to recognize stationary objects but can perceive moving ones. First reported by Riddoch in 1917, known as a feature of cortical blindness.
Blindsight: Unconscious response to visual stimuli despite lack of conscious awareness. Suggests involvement of visual pathways other than LGB-V1 (V2, V3, V4, V5/MT, FST, LIP).
QWhy is the pupillary light reflex normal in cortical blindness?
A
The afferent pathway of the pupillary light reflex goes to the pretectal area of the midbrain before the lateral geniculate body (LGB) and does not pass through the occipital lobe (primary visual cortex). Therefore, even if the occipital lobe is damaged, the pupillary light reflex is preserved. Together with normal fundus findings, this is a characteristic finding of cortical blindness.
The main causes and associated risk factors of Anton syndrome are shown below.
Vascular Causes
Bilateral PCA infarction: The most common cause. Infarction of both posterior cerebral arteries leads to extensive damage to the occipital lobes.
After trauma or tumor: May occur after head injury, brain tumor, or surgery.
Heart surgery or cerebral angiography: Known as iatrogenic risk factors.
Carbon monoxide poisoning or PRES: Can also develop in toxic or reversible posterior leukoencephalopathy syndrome (PRES). Anticancer drugs such as cisplatin are also causes.
Non-vascular causes
MELAS: Mitochondrial encephalomyopathy. Onset has been reported in cases with mt.3243A>G mutation. 2)
MS exacerbation, pregnancy-induced hypertension, obstetric hemorrhage: Secondary to various systemic conditions.
Infectious diseases: West Nile virus (WNV) encephalitis, HIV-associated PML, etc. 3)
Others: Adrenoleukodystrophy, central nervous system vasculitis, ischemia associated with subarachnoid hemorrhage, bilateral optic radiation lesions in Trousseau syndrome, etc.
An anatomical feature of the posterior cerebral artery (PCA) is that it branches from the basilar artery, with the proximal segment (P1–P2) supplying deep structures (posterior thalamus and midbrain) and the distal segment (P3–P4) supplying the occipital cortex. Damage to the P4 segment is the main cause of visual field defects. 1) The occipital cortex is located far from the central vascular system and has a structure vulnerable to ischemia.
QCan Anton syndrome occur from causes other than stroke?
A
MELAS (mitochondrial encephalomyopathy) 2), MS (multiple sclerosis), West Nile virus encephalitis 3), trauma, carbon monoxide poisoning, and other diverse non-vascular causes can also lead to onset. In all cases, bilateral occipital lobe dysfunction is the common pathological basis.
Clinical diagnosis is made by combining the following four points: history of confabulation, clinical evidence of vision loss, normal fundus findings, and imaging confirmation of occipital lobe damage.
Head CT (NCCT): Useful for emergency evaluation. Confirms ischemic infarction (low-density area). For example, it appears as an ischemic infarction in the right temporo-occipital lobe. 1)
Head MRI:
DWI is useful in the hyperacute phase (within 6 hours). DWI can detect acute infarcts that are difficult to detect on T1, T2, and FLAIR.
FLAIR images are excellent for distinguishing cerebral infarction from cerebrospinal fluid.
Check for hyperintense signals in the occipital cortex and subcortical white matter on T2-FLAIR. 2)3)
Interpretation of DWI findings: DWI hyperintensity with isointense ADC (no reduction) suggests changes due to epileptic seizures, and is differentiated from ischemic stroke (which shows reduced ADC). 2)
VEP (Visual Evoked Potentials): Useful for confirming complete cortical blindness. It can objectively demonstrate lack of response to stimuli and is also used to differentiate from malingering.
V-EEG (Video EEG): Useful when epileptic seizures are suspected in conditions such as MELAS. Can capture seizures originating from the occipital lobe. 2)
No abnormalities in eyeball or light reflex (common with cortical blindness); psychiatric evaluation required
Differentiation from psychogenic visual disturbance is particularly important. Cortical blindness due to bilateral occipital lobe lesions shows no abnormal findings in the eyeball and preserves the light reflex, so it is easily mistaken for mental illness or malingering.
MS-related: Steroid pulse therapy (IV methylprednisolone) + plasma exchange. Cases have been reported where recovery of insight followed by visual recovery occurred gradually over 2 years.
WNV encephalitis-related: Methylprednisolone 1000 mg/day for 7 days was attempted but did not respond in reported cases; no established treatment exists. 3)
QHow important is the time from onset to treatment?
A
In cases originating from stroke, tPA (thrombolytic therapy) is indicated within 4.5 hours of onset. 1) Beyond this time, prevention of recurrence and rehabilitation become the mainstays of treatment. The more time available, the greater the potential to salvage neurons, so it is important to seek emergency care immediately upon symptom onset.
Bilateral extensive damage to the occipital lobes (primary visual cortex V1) causes bilateral homonymous hemianopia, ultimately leading to cortical blindness. The occipital cortex is located far from the central vascular system and is vulnerable to ischemia. Infarction of the distal posterior cerebral artery (P3–P4) disrupts blood flow to the occipital lobe. 1)
Visual information processing involves the ventral pathway (“what” pathway: area V4, form and color recognition) and the dorsal pathway (“where” pathway: area V5, spatial location and motion recognition). Some subcortical fibers bypass V1 and directly connect to V4 and V5, so even when V1 is extensively damaged, these pathways may function, allowing color perception and motion detection to be preserved. 1) This is the neurological basis of the Riddoch phenomenon (seeing moving objects).
As for the mechanism of blindsight, studies using macaque monkeys have reported direct projection pathways from the LGBd to V2, V3, V4, V5/MT, FST, and LIP, which may explain unconscious visual responses.
Several hypotheses exist regarding the mechanism of anosognosia.
Hypothesis
Content
Evidence
Simultaneous damage to visual cortex and association cortex
Primary visual cortex and visual association cortex are simultaneously damaged, leading to lack of insight into one’s own condition
Clinical picture of extensive occipital lobe lesions
Disconnection syndrome
Parietal white matter lesions disconnect the visual cortex from other areas
Onset in cases with white matter lesions
Disconnection from language centers
The connection between the damaged visual cortex and the functioning language area is severed, causing the language area to generate confabulatory responses without visual input.
The confabulated content includes visual details.
Currently, the “disconnection from language centers” hypothesis is the most supported. It is thought that when feedback from the damaged visual cortex to the language area is interrupted, the language area generates false reports of “seeing.”
QWhy do patients claim to see when they cannot?
A
The most supported hypothesis is the “disconnection from language centers” theory. Damage to the occipital lobe disrupts the feedback circuit from the visual cortex to the language area, causing the language area to generate confabulatory responses of “seeing” without visual input. This is not intentional lying but a neurological phenomenon due to brain circuit damage.
Mechanism in MELAS: Abnormal mitochondria accumulate in the endothelial and smooth muscle cells of small arterioles, leading to capillary proliferation. Epileptic seizures cause rapid energy depletion in the neurovascular unit, resulting in a Todd’s paresis-like condition. The Fryer hypothesis proposes that epileptic seizures trigger stroke-like episodes. 2)
Mechanism of blood-brain barrier (BBB) crossing in WNV encephalitis: Three pathways are hypothesized: passive cellular transport, axonal transport, and inflammation-induced BBB disruption. 3)
7. Latest Research and Future Perspectives (Reports at Research Stage)
A case report by Ziaul et al. (2024) reported that COVID-19 patients have a 3.6-fold increased risk of ischemic stroke, and even mild COVID-19 increases stroke risk to about 1%. 1) High inflammatory response, hypercoagulable state, and medical severity are considered predisposing factors for thromboembolism. Delayed medical consultation during the pandemic was also a problem for strokes in the posterior circulation, including PCA.
Ewida et al. (2021) reported characteristic MRI findings of DWI hyperintensity with ADC isointensity (inconsistent with ischemic changes) in a case of MELAS complicated by Anton-Babinski syndrome. 2) These findings differ from DWI changes in ischemic stroke (accompanied by ADC reduction) and are interpreted as a combination of reversible energy metabolism impairment and hemodynamic changes due to epileptic seizures. Differentiation of DWI findings provides important implications for treatment decisions in MELAS.
Srichawla (2022) reported that interferon alpha and purified immunoglobulin preparations containing WNV antibodies could be future treatment candidates for neuroinvasive WNV infection. 3) Currently, response to existing drugs including methylprednisolone is poor, and no established treatment exists. Over 80% of WNV infections are asymptomatic, but less than 5% progress to neuroinvasive disease, making the establishment of treatment urgent.
Ziaul YH, Mittal J, Afroze T, et al. Anton-Babinski Syndrome: A Visual Anosognosia. Cureus. 2024;16(3):e55679.
Ewida A, Ahmed R, Luo A, et al. Mitochondrial Myopathy, Encephalopathy, Lactic acidosis and Stroke-Like Episodes Syndrome Presenting With Anton-Babinski Syndrome and Concurrent Occipital Lobe Seizures. Cureus. 2021;13(1):e12908.
Srichawla BS. Neuroinvasive West Nile Virus (WNV) Encephalitis With Anton Syndrome: Epidemiology and Pathophysiology Review. Cureus. 2022;14(6):e26264.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.