McArdle disease, also known as glycogen storage disease type V (GSD5), is a metabolic myopathy caused by a complete deficiency of myophosphorylase, impairing muscle glycogen breakdown. It was first reported by Brian McArdle in 1951.
Genetics and Causes
Causative gene: PYGM gene (11q13). Over 100 pathogenic variants have been identified. 1)2)
Inheritance pattern: Autosomal recessive. 1)
Enzyme deficiency: Complete deficiency of myophosphorylase, preventing conversion of muscle glycogen to glucose-1-phosphate. 1)
Epidemiology and Onset
Prevalence: Estimated at 1:100,000 to 1:167,000. 1)
Age of onset: Often occurs during adolescence to young adulthood. 1)
Ophthalmic relevance: Since the RPE expresses the muscle-type phosphorylase isoform, glycogen metabolism disorders can lead to retinal pattern dystrophy.
Main Symptoms
Decreased exercise tolerance: Occurs with both aerobic and anaerobic exercise. 1)
Rhabdomyolysis: More than 50% of patients experience it at least once in their lifetime. 2)
Myophosphorylase is an enzyme that cleaves the outer branches of glycogen to produce glucose-1-phosphate, supplying energy to the glycolytic pathway. 1) When this enzyme is deficient, muscles cannot use glycogen as an energy source during exercise.
Ophthalmologically, the RPE is known to express muscle-type phosphorylase, and dysfunction of this enzyme is thought to reduce energy supply to the outer retina, leading to retinal pattern dystrophy. Additionally, as a general glycogen storage disease, glycogen deposition can occur in the corneal epithelium and retinal vascular pericytes.
QHow rare is McArdle disease?
A
The prevalence is estimated at 1:100,000 to 1:167,000, making it an extremely rare disease. 1) Over 100 pathogenic mutations have been identified in the PYGM gene, and research on genotype-phenotype correlations is ongoing. 2)
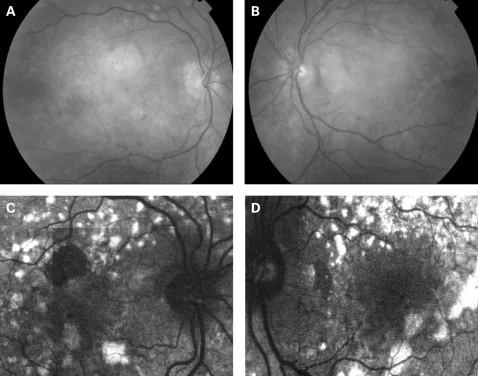
P P Rath; S Jenkins; M Michaelides; A Smith; M G Sweeney; M B Davis; F W Fitzke; A C Bird. Characterisation of the macular dystrophy in patients with the A3243G mitochondrial DNA point mutation with fundus autofluorescence. Br J Ophthalmol. 2008 May 22; 92(5):623-629. Figure 4. PMCID: PMC2569141. License: CC BY.
(A, B) Fundus photographs of patient 10 showing a granular appearance to the RPE. The yellow-white deposits at the level of the RPE are circumferentially oriented and extend just beyond the vascular arcades. The deposits are slightly more prominent in the left eye. In the right eye, there is a small circular patch of perifoveal atrophy present superiorly. (C, D) Fundus AF images of patient 10, 2 years after the fundus photographs. The pale yellow deposits are associated with increased AF oriented in a circular fashion surrounding the macula and optic nerve. There is decreased AF in areas of atrophy and a diffuse abnormality of AF within the macula and surrounding the optic nerve, which is greater than expected, based on the fundus photographs. Patient consent has been obtained for publication.
The main subjective symptoms are muscle symptoms related to exercise. 1)
Decreased exercise tolerance: Occurs with both aerobic and anaerobic exercise. Fatigue easily even with daily activities.
Muscle pain and muscle cramps: Occur during or after exercise. They become noticeable with heavy labor or intense exercise.
Fatigue: May persist as chronic fatigue.
Dark urine (myoglobinuria): When rhabdomyolysis occurs, myoglobin from muscles is excreted in the urine, causing dark urine. 1)2) This is a warning sign of acute kidney failure.
Ophthalmologically, if retinal pattern dystrophy is present, patients may notice mild vision loss or visual field abnormalities.
Rhabdomyolysis is a serious complication experienced at least once by more than 50% of patients. 2) Laboratory abnormalities associated with rhabdomyolysis are shown below.
Test item
Example of abnormal value
Clinical significance
CK
Baseline 1,000–2,000 U/L, tens of thousands U/L or more during an attack
Indicator of muscle damage
Cr
Elevated (e.g., 7.71 mg/dL)2)
Renal impairment
AST/ALT・LDH
Elevated (e.g., LDH 2,145 U/L)2)
Muscle and liver damage
In severe cases, acute renal failure (CK 89,243 U/L, Cr 7.71 mg/dL, LDH 2,145 U/L) and uremic encephalopathy have been reported. 2) Electrolyte abnormalities (hypokalemia) and hyperuricemia are also observed. 2)
Second wind phenomenon is a characteristic finding of this disease. Symptoms decrease about 10 minutes after starting exercise, allowing the patient to continue exercising again. 1) Details are explained in the “Pathophysiology” section.
Ophthalmic findings
Pattern dystrophy of the retina: Observed in the fundus as yellow reticular lesions. Changes at the RPE level are predominant.
RPE atrophy and loss of photoreceptor outer segments: Seen in advanced cases.
QWhat is the second wind phenomenon?
A
The second wind phenomenon is a phenomenon in which muscle pain, muscle cramps, and fatigue that were felt until about 6 to 10 minutes after the start of exercise are alleviated, allowing the person to continue exercising again. 1) This phenomenon occurs because blood-derived glucose and fatty acids are mobilized as energy sources instead of muscle glycogen. For details, see the “Pathophysiology” section.
McArdle disease is caused by a complete deficiency of myophosphorylase due to pathogenic variants in the PYGM gene. 2) Because it is an autosomal recessive disorder, it develops when both alleles have mutations.
The main factors that trigger rhabdomyolysis are as follows. 1)
Strenuous aerobic and anaerobic exercise: the most frequent trigger
Scuba diving: The combination of high-pressure environment, hypothermia, and exercise load can trigger the condition1)
Childbirth: Increased muscle energy demand due to uterine contractions
Anorexia nervosa: Increased muscle fragility due to poor nutritional status
Asthma attack: Overload of accessory respiratory muscles
Alcohol-induced seizures: Tonic contraction of skeletal muscles
Medications: Statins, acetazolamide, etc.
Ophthalmologically, because the RPE expresses the muscle-type phosphorylase isoform, dysfunction of this enzyme reduces energy supply to the outer retina, posing a risk for retinal lesions.
QWhat activities can cause rhabdomyolysis?
A
Strenuous exercise is the most common trigger, but scuba diving, childbirth, anorexia nervosa, asthma attacks, and alcohol-induced seizures can also be triggers. 1) Medications such as statins and acetazolamide also increase the risk of rhabdomyolysis, so it is necessary to inform your doctor when prescribed.
Diagnosis is made through a combination of clinical symptoms, biochemical tests, muscle biopsy, and genetic testing.
Test
Main Findings
Diagnostic Significance
Muscle biopsy
Phosphorylase deficiency
Definitive
Genetic testing
PYGM mutation
Definitive
CK・LDH
Baseline elevation
Auxiliary
Muscle biopsy
Peripheral anterior synechiae (periodic acid–Schiff staining) confirms glycogen accumulation, and subsarcolemmal blebs are observed as characteristic findings. 2) Phosphorylase histochemical staining shows loss of enzyme activity.
Biochemical testing
CK, LDH, and transaminases (AST/ALT) show baseline elevation even at rest. 1)2)
During rhabdomyolysis attacks, evaluate acute renal failure indicators (elevated Cr, hyperuricemia) and electrolyte abnormalities (hypokalemia). 2)
Electrophysiological Testing
EMG (electromyography) may show mild myopathic findings. 2)
Genetic Testing
Sequence analysis of the PYGM gene identifies pathogenic variants. It can be compared with over 100 known mutations.
Ophthalmic examination
Fundus examination and FAF are used to evaluate retinal pattern dystrophy. After a definitive diagnosis, regular fundus examinations are recommended.
QHow is McArdle disease diagnosed?
A
The gold standard is confirmation of phosphorylase deficiency by muscle biopsy. 2) Characteristic findings include glycogen accumulation and subsarcolemmal vacuoles on periodic acid–Schiff staining. PYGM genetic testing is also used for definitive diagnosis. In biochemical tests, elevated resting CK is useful as an auxiliary diagnostic aid, and during episodes of rhabdomyolysis, assessment of renal function and electrolytes is necessary. 1)2)
Supervised exercise program: Gradually improve aerobic capacity under professional guidance. 2)
Dietary management: A high-complex carbohydrate, low-fat diet is recommended. 2)
Pre-exercise sucrose intake: Sugar supplementation just before exercise is considered effective in reducing symptoms. 1)
Ophthalmic management
Regular fundus examination: Periodically monitor the progression of retinal pattern dystrophy.
FAF examination: Evaluate changes in autofluorescence patterns over time.
No established treatment: No specific treatment for retinal lesions has been established at present.
Acute phase management
During an attack of rhabdomyolysis, large-volume intravenous fluid resuscitation is the highest priority treatment. 1)2) Strict management of fluid volume, urine output, and electrolyte balance is essential to prevent acute kidney injury. In severe acute kidney injury, emergency hemodialysis may be required. 2)
Long-term management
Supervised exercise program: Gradually improve exercise tolerance. Should be performed under the supervision of a specialist. 2)
Dietary management: A high-complex-carbohydrate, low-fat diet is recommended. 2)
Pre-exercise sucrose intake: Consuming sugar (sucrose) immediately before exercise may help reduce symptoms. 1)
Normally, muscle glycogen is converted to glucose-1-phosphate by muscle phosphorylase and used for ATP production via glycolysis. 1) In McArdle disease, this pathway is completely blocked, severely limiting anaerobic energy supply immediately after the start of exercise. 2)
As a result of muscle energy deficiency, the following molecular mechanisms cause rhabdomyolysis. 2)
Decreased Na/K pump activity: Impaired maintenance of membrane potential
Increased intracellular Ca²⁺: Excessive muscle contraction and cell membrane damage
Increased oxidative stress: Increased production of reactive oxygen species
As a result, the muscle cell membrane breaks down, and myoglobin, CK, and LDH leak into the blood.
Approximately 6 to 10 minutes after the start of exercise, blood-derived glucose (from liver glycogen) and free fatty acids (from adipose tissue) are mobilized as energy sources for muscles. 1) This improves the energy state of the muscles and reduces symptoms. This phenomenon is specific to McArdle disease and has diagnostic value.
During scuba diving, the combined effects of high-pressure environment, hypothermia, and exercise load reduce muscle oxygen supply, further increasing the risk of rhabdomyolysis. 1)
McCann and Park (2023) reported a case of a patient with McArdle disease who developed rhabdomyolysis after scuba diving. 1) It is suggested that the high-pressure and hypothermic environment during diving further restricts oxygen supply to muscles, triggering rhabdomyolysis with milder exercise than typical cases.
RPE expresses the muscle-type phosphorylase (PYGM) isoform. When PYGM deficiency impairs glycogenolysis in the RPE, nutrient supply to the outer retina decreases, leading to insufficient energy for photoreceptor outer segment turnover and the phototransduction cycle. This mechanism is thought to underlie the pathogenesis of retinal pattern dystrophy.
QWhy does the eye (retina) also become abnormal?
A
The retinal pigment epithelium (RPE) of the eye expresses the same type of phosphorylase (PYGM) as muscle. Therefore, in McArdle disease, glycogenolysis is also impaired in the RPE, reducing energy supply to the outer retina. This is thought to result in RPE atrophy and loss of photoreceptor outer segments, leading to retinal pattern dystrophy.
7. Latest Research and Future Perspectives (Reports at the Research Stage)
McCann and Park (2023) analyzed in detail a case of rhabdomyolysis in McArdle disease caused by scuba diving, reporting the effects of high pressure, hypothermia, and hyperoxia on muscle energy metabolism. 1) In particular, the possibility that high-concentration oxygen (nitrox 36%) diving may reduce muscle fatigue was mentioned, and research is progressing toward establishing activity guidelines for special environments.
Over 100 PYGM mutations have been identified to date, 2) and research is underway to clarify the association between specific mutations and clinical phenotypes (frequency and severity of rhabdomyolysis, presence of ophthalmic complications). Elucidation of genotype-phenotype correlations is expected to lead to applications in personalized medicine.
Research on the association with retinal pattern dystrophy
Research continues to further elucidate the pathogenesis of retinal degeneration associated with McArdle disease by clarifying the function of muscle-type phosphorylase in the RPE. Although the development of specific interventions for retinal lesions is expected in the future, it remains at the research stage at present.
McCann UG 3rd, Park T. Rhabdomyolysis in McArdle disease caused by scuba diving. BMJ case reports. 2023;16(10). doi:10.1136/bcr-2023-255192. PMID:37852664; PMCID:PMC10603480.
Hamadeh M, Nasrallah K, Ajami Z, Zeaiter R, Abbas L, Hamadeh S, et al. Clinical Presentation and Management of Severe Acute Renal Failure in McArdle Disease. Clinical medicine & research. 2021;19(2):90-93. doi:10.3121/cmr.2021.1641. PMID:33985978; PMCID:PMC8231694.
Migocka-Patrzałek M, Elias M. Muscle Glycogen Phosphorylase and Its Functional Partners in Health and Disease. Cells. 2021;10(4). PMID: 33924466.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.